

Carotid Endarterectomy



This is a preview. Check to see if you have access to the full video. Check access
Carotid Endarterectomy: Principles of Exposure, Arteriotomy and Patch Grafting
Carotid endarterectomy (CEA) is one of the most scrutinized surgical procedures in neurosurgery. Large trials have demonstrated definitive benefit in select patients with both symptomatic and asymptomatic carotid stenosis.
Although many trials have been conducted about the effect of carotid endarterectomy in asymptomatic patients, three trials (The Veterans Administration Cooperative Study [VA], The Asymptomatic Carotid Surgery Trial [ACST], and the Asymptomatic Carotid Atherosclerosis Study [ACAS]) represent the bulk of the data in favor of CEA in this setting.
- VA randomized 444 asymptomatic male veterans with carotid stenosis between 50% and 99%. All patients underwent conventional angiography for diagnosis and were treated with aspirin. One group underwent CEA in addition to the aspirin, while the other received only medical management. The primary outcome was an ipsilateral neurologic event.
- ACAS randomized 1662 asymptomatic patients (over 39 North American centers) who had carotid stenosis of at least 60%. The diagnosis was made by angiography or other noninvasive tests (ultrasound, magnetic resonance imaging [MRI], etc.). Patients were randomized to surgery and a daily aspirin or to a daily aspirin alone. Angiography was required before surgical intervention. Primary outcomes included ipsilateral stroke, perioperative stroke, or death.
- ACST randomized 3120 asymptomatic patients with at least 60% carotid stenosis. Like ACAS, diagnosis was made via angiography or other tests such as MRI or ultrasonography. Patients were randomized into an “immediate surgery” group or a “medical group” in which surgery was performed if the patient became symptomatic. As a result, ACST was a trial that assessed the difference between immediate and delayed (until symptoms develop) surgery.
In summary, these trials demonstrated a 29% relative risk reduction in the surgical group for patients with carotid stenosis of at least 60%. This benefit assumes a 3% rate of surgical complications (including angiography).
The data for symptomatic carotid stenosis also favors carotid endarterectomy in certain groups of patients. These data come from two major trials, the European Carotid Surgery Trial (ECST) and the North American Symptomatic Carotid Endarterectomy Trial (NASCET):
- ECST randomized 3024 symptomatic patients to two groups. One group underwent carotid endarterectomy as soon as possible. The other group was given best medical treatment for as long as possible, delaying surgery until absolutely needed. Symptomatic status was granted for patients with evidence of a cerebral ischemic event within 6 months of entry into the study for which the symptoms were ipsilateral to the side of the relevant carotid stenosis.
- NASCET randomized 2926 symptomatic patients into medical or surgical arms. A cerebral ischemic event was considered symptomatic if it occurred ipsilateral to the stenosis in question within 4 months of inclusion into the study.
Pooled together, both trials strongly support endarterectomy for patients with 70% to 99% carotid stenosis. CEA for symptomatic stenosis between 50% and 69% was also supported, albeit less strongly. This finding was based on the fact that the risk of surgery did not change, whereas the risk of primary outcome (ipsilateral stroke) was less in patients with this degree of stenosis treated in the medical arm.
Continued evolution of endovascular technology has brought stenting of carotid stenosis to the forefront. Yet, major trials have not proven (although these trials are still ongoing) these new technologies superior to endarterectomy in the treatment of asymptomatic and symptomatic carotid stenosis. As a result, carotid endarterectomy remains an important part of cerebrovascular neurosurgery; neurosurgeons should secure the durability of its application.
Diagnosis
Asymptomatic carotid stenosis is often diagnosed incidentally during diagnostic workup for other complaints. It may be discovered on the contralateral side in a patient who has already been screened for ipsilateral symptomatic carotid stenosis. It is frequently found during evaluation for transient ischemic attacks and stroke. It may also be detected after a carotid bruit is noted on routine physical examination.
Symptomatic carotid stenosis is defined by symptoms in a cerebral territory referable to the ipsilateral hemisphere. Isolated right (nondominant) carotid stenosis may not become symptomatic. Variations and caveats abound in this discussion and are beyond the scope of this chapter.
In general, the NASCET measurements have been used to objectively determine the extent of stenosis. The diameter of the lumen at the greatest point of stenosis serves as the numerator, while the diameter of the internal carotid artery (ICA) above the bulb and beyond the stenosis serves as the denominator. ECST measured the point of greatest stenosis in relation to the diameter of the carotid bulb at the same point as the stenosis. ECST measurements often overestimate the same stenosis measured by means of the NASCET criteria.
Evaluation
Patients with carotid stenosis require comprehensive medical evaluation. Imaging of the carotid vasculature is required. Although ultrasound is a reasonable study for periodic assessment and follow-up/surveillance imaging, it is generally not adequate for surgical planning. I have also found that MRA has a tendency to overestimate the degree of stenosis. As a result, computed tomography angiogram (CTA) of the head and neck or catheter angiogram are my preferred modes of diagnosis. The presence of tandem stenoses at the level of the intracranial ICA should be excluded as CEA alone is unlikely to be beneficial in these special cases.
Once the clinical examination has been documented and appropriate imaging has been obtained, a determination of the type of stenosis (symptomatic versus asymptomatic) can be made. This information allows appropriate risk stratification and patient counseling when discussing the risks and benefits of proceeding with an endarterectomy.

Figure 1: A high-grade left-sided carotid stenosis caused by an ulcerated, partially calcified plaque is evident on the preoperative catheter (left image) and CT angiogram (right two images-arrows).
Indications for the Procedure
As discussed above, the existing literature supports CEA for both symptomatic and asymptomatic patients. For symptomatic patients, CEA is advisable for 50% to 99% stenosis. Patients with stenosis greater than 70% benefit the most. There are no data to support revascularization of a completely occluded carotid artery and is not recommended due to the risk of distal embolization.
Patients with asymptomatic carotid stenosis can benefit from surgery if they have stenosis greater than 60%. Because the benefit of CEA among asymptomatic patients does not favor surgery until 2 to 3 years after intervention, the patients’ medical comorbidities should be carefully considered because CEA may not be beneficial in all asymptomatic patients.
I recommend endovascular stenting to patients with medical comorbidities that preclude the use of anesthesia. There is no class I evidence to support the superiority of stenting over surgery.
Preoperative Considerations
There are multiple preoperative considerations that must be taken into account before CEA. The height of the bifurcation will determine the extent of exposure necessary to complete the operation. The bifurcations that are higher than C2 vertebral body may not be readily exposable through the neck incision and endovascular options may be explored. Assessment of the patient’s neck mobility is important.
Preoperative assessment of the patient’s intracranial vasculature is also important. This includes evaluation of the anterior and posterior communicating arteries for providing collateral flow during intraoperative cross-clamping of the ICA. Intraoperative electroencephalogram (EEG) is used to assess hypoperfusion and therefore a baseline preoperative EEG may be reasonable.
Aspirin is continued perioperatively. I avoid the use of Plavix (clopidogrel) during this period due to the added risk of postoperative hematoma accumulation. Patients who are on Coumadin are admitted to the hospital and placed on intravenous heparin therapy for normalization of their prothrombin time. Heparin drip is continued until the time of arteriotomy closure in the operating room and withheld for 48 hours, after which Coumadin is reinstituted.
All patients undergo medical evaluation before surgery because many of them suffer from cardiac disease, diabetes and intractable hypertension.
Instrumentation
The use of a single set of instruments that includes all the necessary items, eliminating the need for refamiliarizing the different surgical teams, is essential. My particular instrument set includes four (two large and two small) vascular pickups, special dissecting scissors, micro ring-tipped forceps (for cleaning the small flaps from the artery wall), and cross-clamps, shunt clamps, and needle drivers. There are various commercial kits available for this purpose.
Operative Anatomy
Carotid endarterectomy takes place in the anterior triangle of the neck. The borders of this triangle include the sternocleidomastoid muscle posteriorly, the trachea-esophageal complex anteriorly, and the lower border of the mandible superiorly. The apex is located at the sternal notch where the sternocleidomastoid muscle and midline converge.
There are several anatomical relationships that help guide the dissection. First, the jugular vein lies lateral to the carotid artery. If the patient’s head is rotated contralaterally too far, the vein may lie on top of the carotid artery and obstruct the operative corridor.
The anatomy of the external carotid artery (ECA) and its branches are the key landmarks for reaching an appropriate exposure. The ECA arises from the common carotid artery (CCA) lateral to the upper border of the thyroid cartilage. The ECA has eight branches. The superior thyroid is its first branch, and lingual and facial arteries arise from its anterior surface. The occipital and posterior auricular arteries arise from its posterior surface, and the ascending pharyngeal artery arises from its medial surface. The artery ends within the parotid gland at the level of the neck of the mandible by the two terminal branches: maxillary and superficial temporal arteries.
Three nerves are particularly important during this procedure. The hypoglossal nerve crosses the ICA at the distal end of the dissection and must be preserved. Hypoglossal nerve injury is the most common nerve injury during CEA. When the ECA-ICA bifurcation his located too cranially, the risk of hypoglossal injury increases. The location of the hypoglossal nerve can be discerned by pursuing the ansa cervicalis superiorly where it joins the hypoglossal nerve. Finally, the vagus nerve runs within the carotid sheath, typically along its posterolateral aspect and behind the carotid artery and jugular vein. Careful dissection of the sheath allows gentle release of this nerve laterally and posteriorly.
The level of the carotid bifurcation is variable; however, it generally lies at the level of the third or fourth cervical vertebra, and the length of the stenosis greatly affects the extent of the necessary dissection.

Figure 2: The relationship between the vasculature and the nerves in the neck as related to CEA are summarized. The vagus nerve lies deep to the carotid artery and the hypoglossal nerve crosses the ECA and distal ICA. If the operator is disoriented early in dissection before exposure of the carotid sheath and continues dissection more toward the midline (most often related to too much head turn) onto the pharyngeal muscles, postoperative swallowing difficulty is likely. This complication should be avoided by lateral redirection of the dissection along the medial belly of the sternocleidomastoid muscle without injuring the jugular vein.

Figure 3: Gentle lateral mobilization of the internal jugular vein exposes the carotid bifurcation. Branches of the ECA, including the superior thyroid artery, lingual, and facial arteries are marked. Note that the vagus nerve can have a wandering route and should be carefully watched for along the anterior ICA and the jugular vein.
In about 10% of patients, the ICA is medial to the ECA; this anatomical variant should be recognized on preoperative imaging and surgical dissection should be directed medial to the ECA. There is no reason for the operator to confuse the ICA for ECA in these cases.
CAROTID ENDARTERECTOMY
The patient is positioned supine on the operating room table with a shoulder roll (bump) laid transversely under the shoulders. This maneuver provides for gentle neck extension to open the operative space between the chin and clavicle. A piece of tape may be used to provide gentle traction on the mandible, allowing for increased exposure, especially in cases involving high bifurcations or plaques.
A slight turn of the patient’s head toward the opposite side can help expose the anterior triangle of the neck. This turn should not be more than 20 degrees because further turn will move the sternocleidomastoid muscle over the carotid sheath and interfere with the exposure.
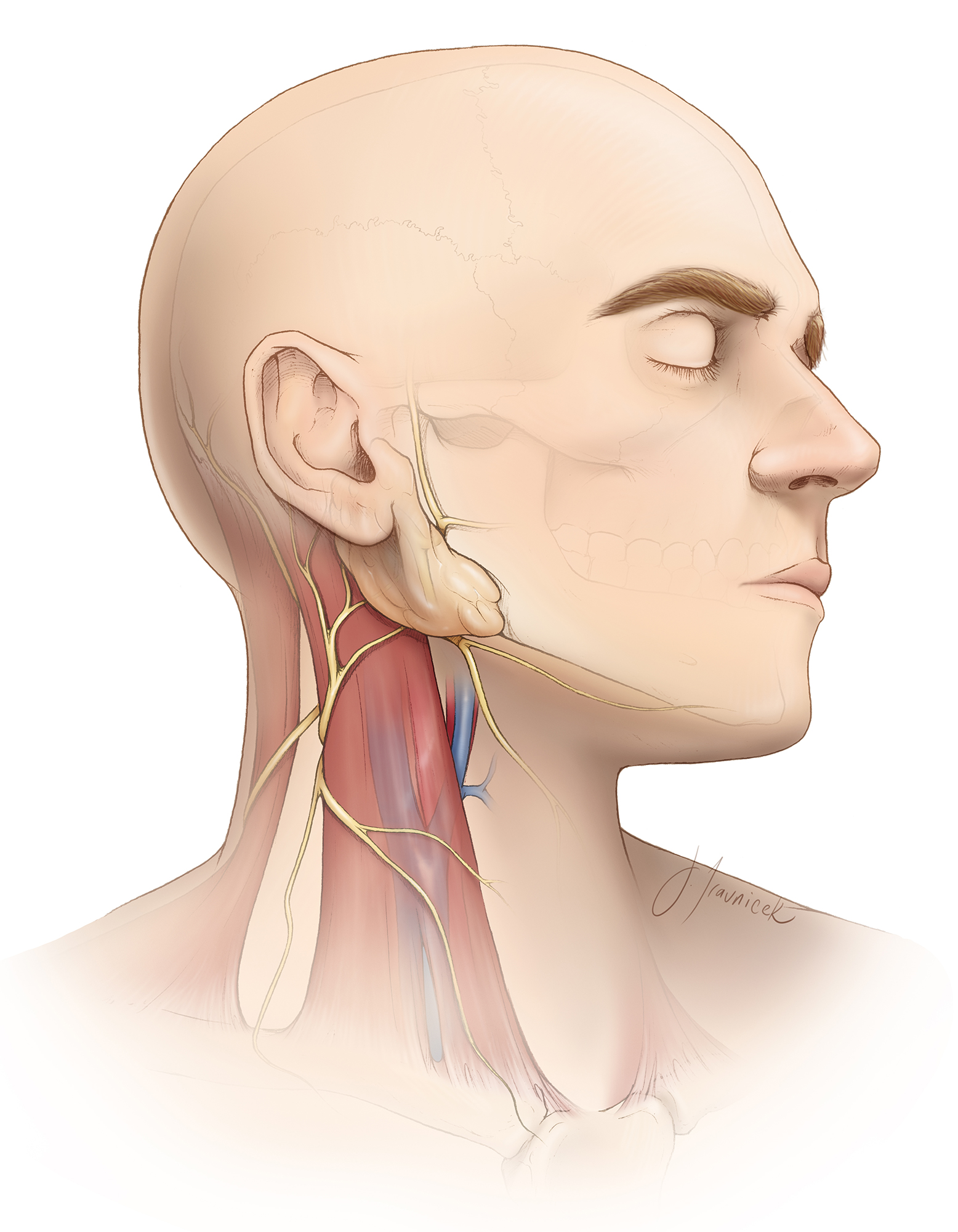
Figure 4: The anatomic relationship between the sternocleidomastoid muscle and jugular vein is the key landmark for reaching the carotid arteries. The marginal mandibular branch of the facial nerve is especially at risk during dissection and retraction of the soft tissues around the angle of the mandible. Its palsy will lead to an asymmetrical postoperative smile upon elevation of the lower lip on the affected side. This weakness is temporary.
Incision and the Initial Exposure
The attachments of the sternocleidomastoid muscle (SCM) are betrayed by its name and each serves an important purpose. The mastoid tip should be palpated and represents the direction in which the incision may be extended if higher exposure is needed.
The level of the bifurcation and necessary exposure (based on the location and length of the plaque) may be estimated via surface landmarks. The thyroid cartilage approximates the level of C4-5. Since almost all bifurcations occur above this level, the incision should travel above it. The angle of the mandible and the hyoid bone approximate C3, while the inferior teeth represent C2.
The incision for a carotid endarterectomy is often tailored to the location of the underlying plaque. Low bifurcations with focal plaques often lend themselves well to transverse incisions along the creases of the neck to enhance cosmesis. This type of incision is similar to the incision used for an anterior cervical discectomy procedure.
Carotid bifurcations often require more exposure if they are significantly diseased, have a long segment of plaque, or are higher within the anterior triangle of the neck. This can be accomplished through a slightly curved or straight incision along the anterior margin of the sternocleidomastoid muscle. I use a subcutaneous injection of 1% lidocaine with 1:100000 epinephrine for local anesthesia and hemostasis before the incision.

Figure 5: A vertical incision is made extending from just above the angle of the mandible to just below the thyroid cartilage, along the anterior border of the sternocleidomastoid muscle (top image). The incision may be enlarged as low as the suprasternal notch and as high as the retroauricular region, depending on the level of the bifurcation. The incision should not closely approach the angle of the mandible to decrease the risk of marginal mandibular branch injury. The angle of the mandible and the sternal notch are marked (bottom photo). Note the slight rotation of the patient’s neck.
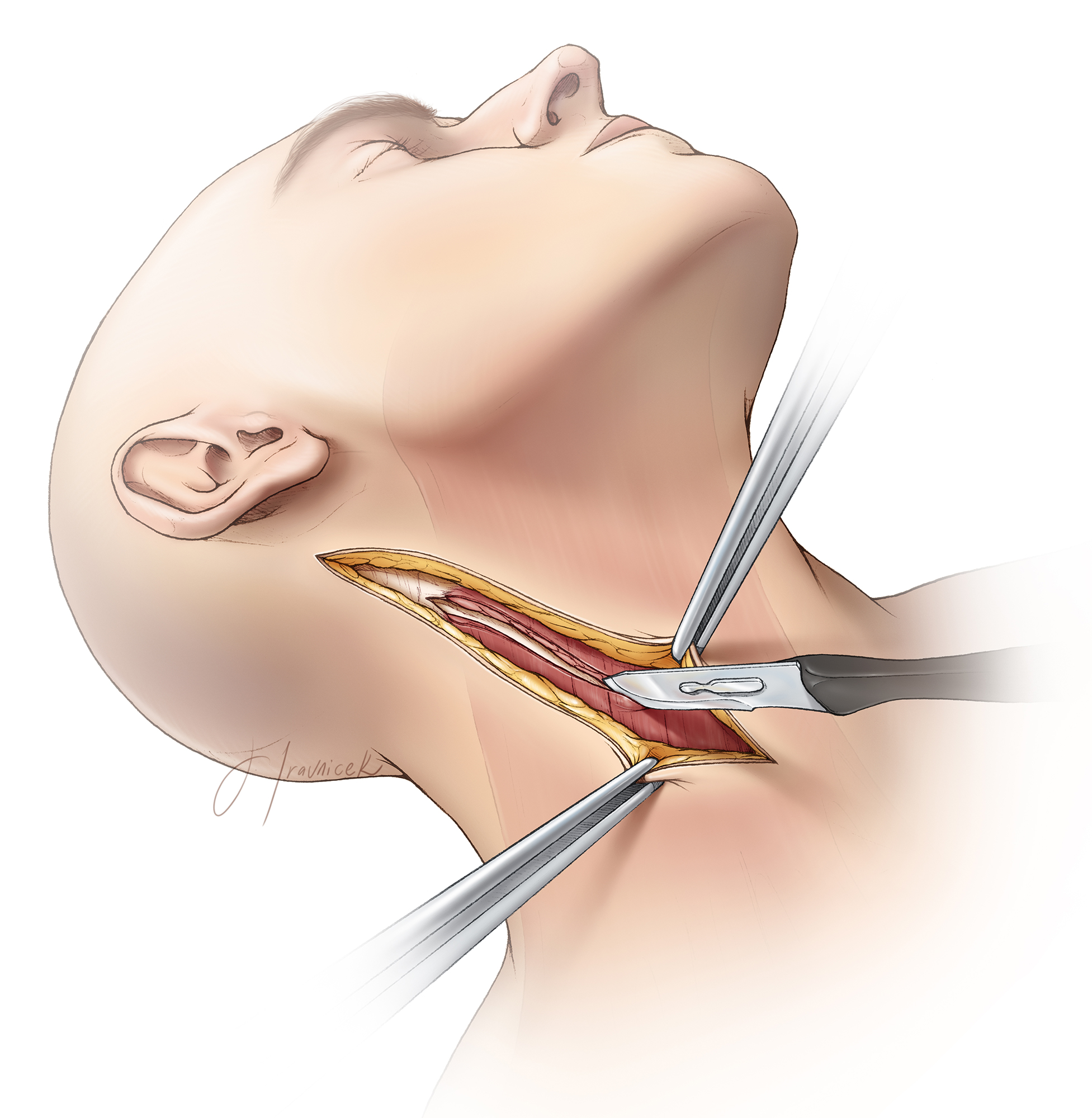
Figure 6: The initial incision is shallow, taken down only to the level of the platysma muscle. Next, the subcutaneous tissue and platysma are divided parallel to the incision. I use a #10 scalpel-size knife to transect the platysma, whereas most operators use the spreading motion of the Metzenbaum scissors to free the muscle from any underlying attachments before its transection. Monopolar electrocautery is used to transect the mobilized muscle while avoiding any damage to the underlying veins. Often the external jugular vein lies just beneath the platysma and may require suture ligation; ignoring this vein can lead to brisk venous bleeding.
The transverse cervical nerve is transected in the above process. This maneuver leads to numbness over the anterior neck area that resolves in 3-6 months.
Once the platysma is divided, the anterior edge of the sternocleidomastoid muscle should be discernible. The dissection proceeds in the soft tissue plane along the medial belly of the sternocleidomastoid muscle; I follow the medial surface of this muscle while gently reflecting the muscle laterally. Wandering dissection deep to the neck region while not pursuing the medial surface of the muscle leads to swallowing dysfunction caused by injury to the recurrent laryngeal nerve (located in the trachea-esophageal groove) and potentially pharyngeal muscles.

Figure 7: Upon gentle lateral reflection and retraction of the sternocleidomastoid muscle, I palpate the soft tissues along the medial aspect of its belly for the pulse and the location of the carotid artery. Note the direction of the palpation just along the medial surface of the muscle (top image). Division of the soft tissue planes between the sternocleidomastoid muscle and the midline swallowing muscles identifies the jugular vein. Fish-hook retractors may be employed to expand this plane, but the recurrent laryngeal nerve or the esophagus should not be injured by the hooks or retractor blades (bottom image).

Figure 8: During the next step, blunt dissection within the potential space parallel to the medial surface of the sternocleidomastoid muscle exposes the common facial vein (top image). Large venous tributaries may join the jugular vein within this part of the operative field; the most dominant of these veins is the common facial vein. The jugular vein must be mobilized laterally, requiring division of these veins. Large tributaries require suture ligation via 2-0 silk sutures (bottom image). Once freed, I use the stump of the transected vein(s) underneath the retractor blades or fish-hooks to displace the jugular vein and expose the carotid sheath. The hooks or blades should not directly injure the large vein. All the nerves medial to the jugular vein, including the ansa cervicalis, are preserved.
Exposure of the Carotid Artery
Using the spreading action of the scissors, I dissect the soft tissue planes between the jugular vein and the carotid artery, laterally mobilize the jugular vein, and unveil the carotid sheath. Continued spreading dissection using a Tonsil clamp further isolates the carotid sheath; its sharp vertical incision exposes the underlying carotid artery.
Two nerves, the ansa cervicalis and the vagus nerve, should be identified during this dissection process. The vagus nerve usually travels along the deep and lateral surface of the carotid artery (in the groove between the carotid artery and jugular vein), but can have wandering routes. Regardless, I do not dissect the nerve, but some operators advise its mobilization free from its medial attachments so that it may be released laterally with the jugular vein. The ansa cervicalis can be pursued superiorly, along with the carotid artery itself, serving as a roadmap to the location of the hypoglossal nerve.

Figure 9: Division of the carotid sheath is illustrated (top image). Next, the carotid artery is dissected circumferentially free of its sheath using the continuous spreading action of a Tonsil clamp. The common facial vein, ansa cervicalis, and the hypoglossal nerve are depicted (lower photo). Preservation of the normal anatomy is the goal.
The dissection of the carotid sheath begins with the exposure of the common carotid artery (CCA). Depending on the level of the bifurcation, this exposure may require retraction (by way of a retention suture) or division of the omohyoid muscle. Distal dissection of the internal carotid artery (ICA) will expose the hypoglossal nerve. Enough dissection has been established when there is adequate room for the arteriotomy, vessel loop, and a small low closing force bulldog clamp around the ICA just above the border of the plaque, and a vessel clamp (large soft-shoe Fogarty vascular clamp) around the CCA. The length of the plaque (determined through gentle palpation of the arterial wall using a moistened finger) also affects the extent of appropriate exposure.
The dissection continues along the anterior aspect of the ICA. The length and location of the plaque may dictate more rostral exposure; care must be taken to avoid injuring the hypoglossal nerve. As stated above, the ansa cervicalis can serve as a guide to the location of the hypoglossal nerve. The hypoglossal nerve is typically located along and directly over the rostral ICA, crossing this artery in an orthogonal direction as the nerve proceeds toward the mandible. If rostral mobilization of the hypoglossal nerve is necessary, the ansa cervicalis can be transected where it joins the hypoglossal nerve to untether the latter nerve. The hypoglossal nerve is then retracted using a vessel loop.
A small arterial branch of the ECA to the sternocleidomastoid muscle rarely requires coagulation and transection to facilitate adequate mobilization of the hypoglossal nerve. If a high exposure is mandatory, the posterior belly of the digastric muscle may be transected without any untoward consequences.
I rarely inject the carotid sinus with approximately 2cc of 1% Xylocaine using a 25-gauge needle, only if significant hemodynamic instability during vessel manipulation and dissection in the region of the bifurcation are noted. The benefits of this maneuver are debated.
Lastly, the ECA is exposed circumferentially around its proximal end. Unlike the other two arteries, only a small segment of the ECA, just distal to the bifurcation, should be released. This maneuver includes identification of the superior thyroid artery. This limited exposure ensures that the ascending pharyngeal artery, not often directly visualized within the operative field, will be gathered up in the tissue distal to the ECA exposure and will, therefore, be excluded from the circulation when a clamp or vessel loop is placed around the ECA.
Prearteriotomy Dissection
It is not enough to simply expose the three major segments of the carotid artery. Once dissected on their superficial surface, circumferential isolation of the CCA, ICA and ECA is important. Such circumferential dissection provides the operator with an opportunity to rotate the artery (if needed) into a more favorable angle for the arteriotomy. It also allows for manipulation of the artery during clamping, ensuring that the entire vessel is included within the clamp and the vessel loops are encircling the artery without placing other structures, including the vagus nerve, at risk.
The superior laryngeal nerve is situated deep to the distal ICA and should not be accidentally damaged during dissection.
Following circumferential isolation of the arteries, vessel loops are wrapped twice around each major arterial branch, secured using small Tonsil clamps under no tension and not attached to the drapes. I typically place a long straight aneurysm clip on the superior thyroid artery. Even though the CCA, ICA and ECA are ready for the placement of their final occluding clamps, I take a moment and discuss the next steps regarding necessary instruments, EEG monitoring, and administration of intravenous heparin with the rest of the operating room staff.
A Rummel tourniquet may be used around the CCA and pulled through a rubber sleeve. This maneuver allows constriction of the vessel around an intraluminal shunt, should the need arises. Mosquito clamps on the ends of the vessel loops or Rummel tourniquet hang over the retractor handles.

Figure 10: I incise the carotid sheath parallel to the axis of the ICA and place the lateral edges of the sheath under tension using the fish-hooks or four sutures. This key maneuver elevates the ICA out of its groove closer to the surgeon, and remarkably eases the later steps and working angles of the operation. Long vascular clamps (long aneurysm clips or bulldog clamps) are placed distal to the vessel loops on the ICA, and a Fogarty vascular clamp is placed on the CCA proximal to the plaque. The vessel loops on the ICA hold the ICA clamp in position. A vessel loop on the ECA is adequate for its occlusion. The ICA is occluded first.
Typical heparin doses range from 5000 to 8000 units, depending on the patient’s weight. Adequate time (3-5 minutes) is allowed to ensure the drug reaches its effect before the clamps are applied. A vascular shunt should be available. Additionally, the microscope should be draped during this time.
I prefer to use the microscope for the next stages of the operation, including the arteriotomy, plaque dissection, and vessel closure. Although its use adds time to the procedure, the improved visualization leads to more effective plaque removal and desirable arteriotomy closure.
Arteriotomy
Under the microscope, a long aneurysm clip or small bulldog clamp is placed on the distal ICA, distal to the corresponding vascular loop. Placement is adequate if the entire section of the diseased vessel and a short length of normal vessel are available for the endarterectomy; the exposure of this short length of normal vessel is imperative to avoid suboptimal arterectomy during the later stages of the operation. This clamping is announced to the operating room team and timing begins. The CCA and ECA as well as the superior thyroid artery are also occluded.
Any alterations in EEG recordings require immediate attention and may indicate the need for a vascular shunt. However, most often, an increase in systolic blood pressure of approximately 20% will relieve the EEG changes.
If an increase in blood pressure is inadequate to address the EEG concerns, a vascular clamp is then placed within the CCA and ICA, proximal and distal to the plaque, respectively. Either a vascular loop or a second more robust aneurysm clip can be used to occlude the ECA and superior thyroid artery.
For placement of the shunt, the ICA is cannulated first, and the shunt is secured in place by pulling up on vessel loops; a mosquito clamp is used to hold the rubber sleeve in place. The shunt tubing is collapsed via heavy vascular forceps. The tubing is then cleared of air by briefly releasing the vascular forceps. Next, the distal end of the shunt is placed within the lumen of the CCA while the bulldog clamp on the CCA is removed. The shunt is then advanced into the CCA as the vessel loops or a custom clamp secures the shunt in place (Please see below).

Figure 11: Next, the arteriotomy is made using a #11 scalpel in the CCA, just proximal to the plaque. It is imperative to avoid injury to the back wall of the artery during this maneuver. Any such injury requires a repair of the tear and significantly lengthens the clamp time. If continuous bleeding within the lumen is noted, the closure of the clamps and tension/traction of the vessel loops should be inspected to ensure absence of back flow. Most often, the traction on the vessel loop on the ECA needs to be increased.
Other common causes of intraluminal bleeding include a large ascending pharyngeal artery that was not excluded with the rest of the ECA circulation. Moreover, the ICA clamp may not be tight enough or not spanning all the way across the vessel. Rather than guessing, each vessel loop should be individually tightened, one at a time, to identify which artery is the source of bleeding.
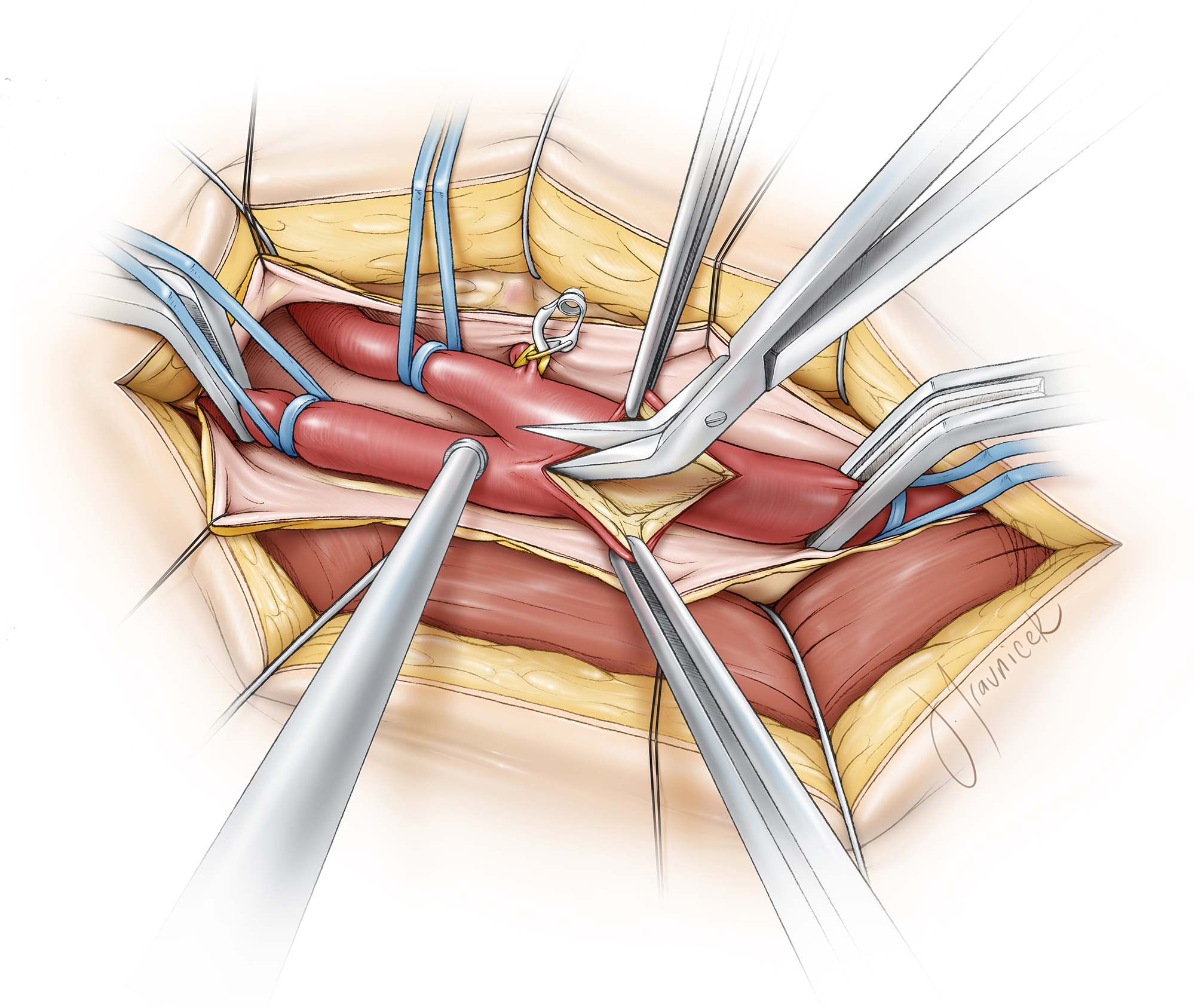
Figure 12: Potts angled scissors are used to complete the arteriotomy through the full extent of the plaque. The arteriotomy should be in line with the center of the bifurcation and ICA. There is a tendency to steer toward the bifurcation initially, and toward the lateral side of the ICA more distally. The more centered the arteriotomy is, the easier will be the performance of the arterial wall closure. The arteriotomy route may be marked using a sterile marking pen.
Calcified plaques can create a special challenge because the scissors may be ineffective. In these situations, I use a #11 scalpel to carefully cut and break through the plaque. Extremely stenotic arteries may present a similar challenge because the scissors’ blades may not have enough space to transverse through the stenotic lumen. The #11 scalpel can also be effective under these circumstances.
It is imperative for the arteriotomy to reach above the plaque in the distal ICA.
Endarterectomy
Dissection of the plaque ideally begins at the proximal end of the arteriotomy within the CCA. It can also begin wherever there is an easily identifiable plane between the plaque and healthy intima and adventitia. I often continue dissecting along one plane; when this plane becomes more difficult to maintain, I switch to another site for the endarterectomy and meet my initial dissection plane later. Aggressive dissection within the arterial wall should be avoided to prevent intimal injuries and tears.

Figure 13: Great care is taken to leave the normal portion of the intima and adventitia intact because the arterial wall can be extremely thin where there is a significant inflammatory response to the atherosclerotic plaque. Dissection is accomplished with the surgeon holding the ipsilateral adventitia while the assistant holds the plaque. Dissection should occur circumferentially around the plaque (inset). Progressively, the plaque is truncated sharply at its distal end, leaving relatively normal intima in the distal CCA and ICA.

Figure 14: Although the loose intimal flaps on the arterial wall at the proximal truncated CCA end of the plaque are unlikely to be a problem because of the direction of blood flow, the same cannot be said for the flaps that are located at the distal end of the arteriotomy within the ICA. Therefore, the distal end of the plaque must be carefully truncated and small free flaps sharply trimmed using microscissors under microscopic magnification. The extent of dissection is adequate distally when the plaque is traversed and relatively normal intima is encountered. There is often a natural line within the ICA where the plaque tends to disconnect itself spontaneously upon gentle traction on the plaque.
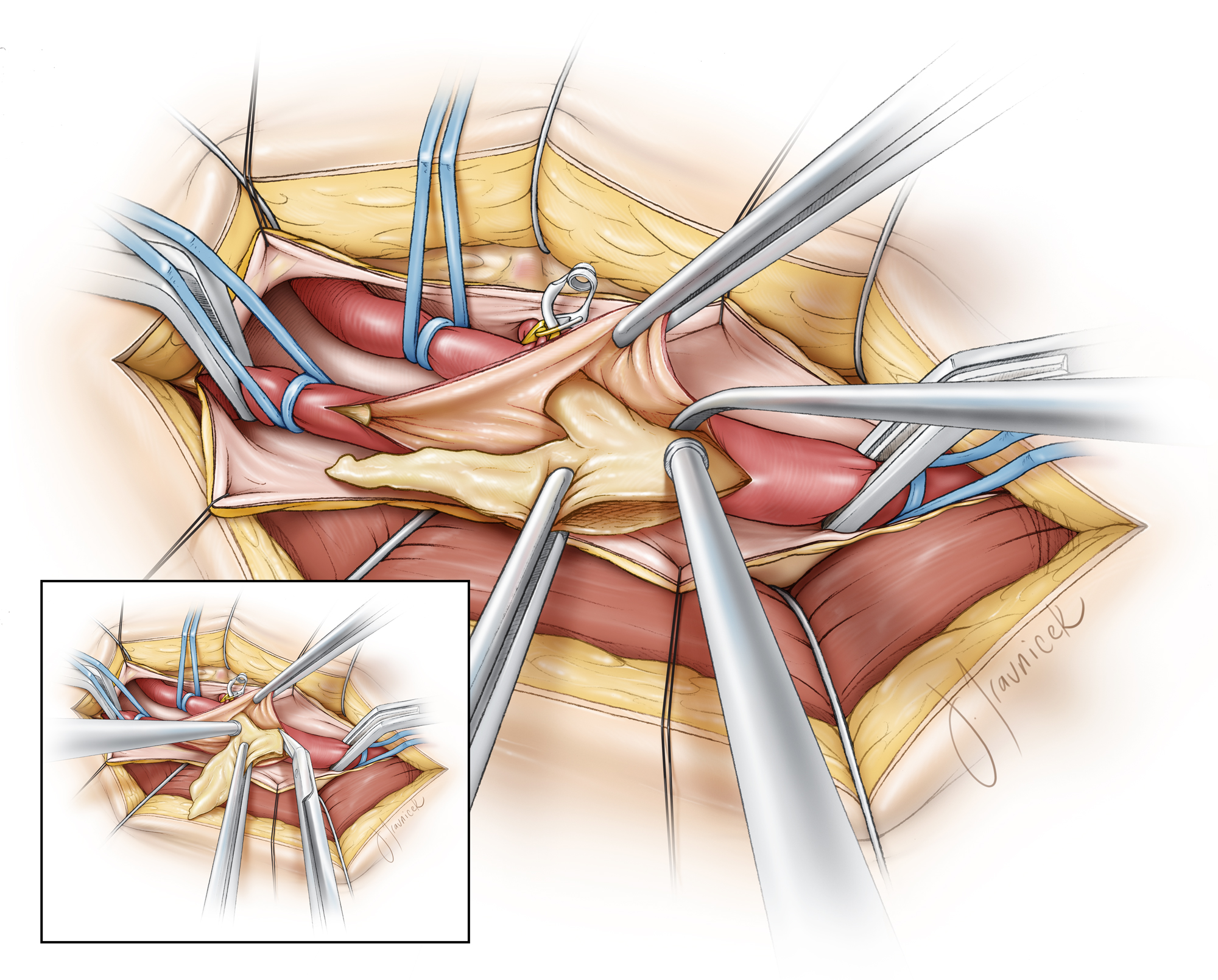
Figure 15. After freeing the plaque distally, I continue the dissection into the CCA and the proximal end of the plaque is disconnected using the Potts scissors. Naturally, the plaque continues into the heart, and therefore a decision must be made to disconnect the plaque at the lower end of the arteriotomy. It is almost impossible to create a clean feathering away of the plaque in the CCA.

Figure 16: Once freed from its distal and proximal ends, the only remaining attachment is within the ECA. After a short segment of the plaque into the ECA is circumferentially exposed, the plaque can simply be pulled away and avulsed from its attachment in the ECA until it is naturally disconnected. This step is often likened to the appearance of a sock being rolled off the foot. The inlet into the ECA has to properly dissected of minor plaque as any thrombus in the proximal ECA can propagate into the ICA and lead to cerebral embolization. If necessary, the arteriotomy may be extended along the wall of the ECA.
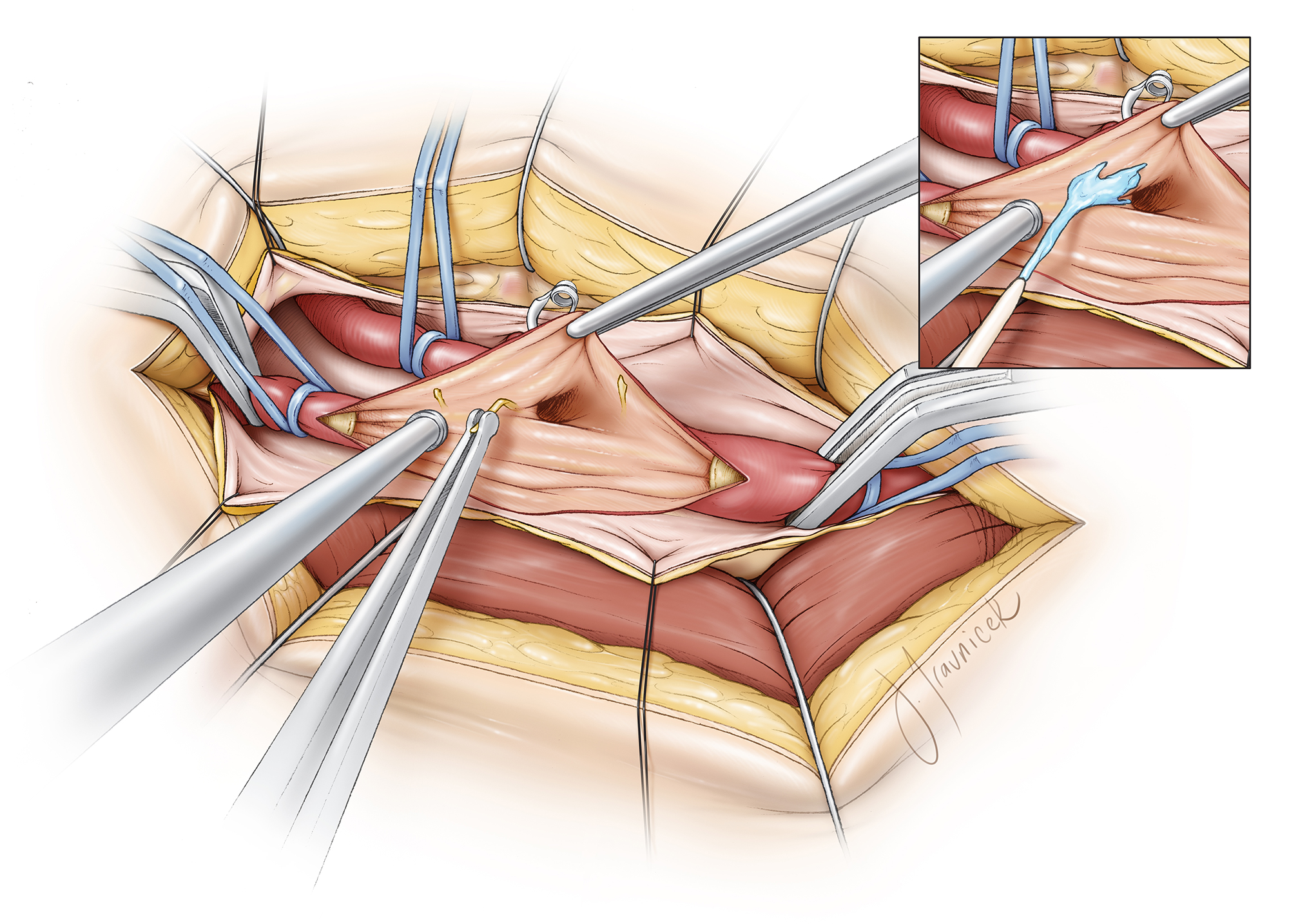
Figure 17: Once the plaque is removed, the remaining intimal surface is carefully inspected and all loose pieces of the intima are removed using micro-ring tipped forceps. Heparin and saline irrigation are used to expose the fine free flaps. The flaps should be stripped away along the entire width of the artery toward the edge of the arteriotomy. Overzealous dissection of the flaps at the distal end of the endarterectomy must be avoided for the fear of extending the intimal damage above the level of the exposure/arteriotomy.
Extending the dissection of the free intimal flaps beyond the arteriotomy along the distal ICA can be problematic. Therefore, back-wall and side-wall flaps should be tacked down with a double-armed unbraided suture (6-0 prolene) if rarely necessary. Both needles must be directed inside to outside so that the knot is tied on the external surface of the vessel. Without this repair, the patient is at risk for arterial dissection once anterograde flow is re-established. Front-wall flaps, on the other hand, can be incorporated into the arterial wall closure.
Closure of the Arteriotomy
Closure of the arteriotomy commences distally with a single-armed 6-0 prolene suture (5-0 may also be selected for larger arteries) in a running fashion. As discussed above, front-wall intimal flaps must be included within the stitch to avoid arterial dissection.
The closure is performed from distal to proximal for about one-half to two-thirds of the arteriotomy. A healthy bite of the arterial wall should be taken on both sides to ensure that the stitch will hold and the irregular edge of the arteriotomy is not exposed to the lumen.
The bite should not be too large, however, to avoid unnecessary constriction of the new lumen, especially at the level of the distal ICA. If the arterial walls are significantly everted, the bites are too big. In most cases, the likelihood that the lumen will be constricted beyond a diameter smaller than the original lumen prior to plaque removal is low, especially at the level of the bifurcation and CCA.
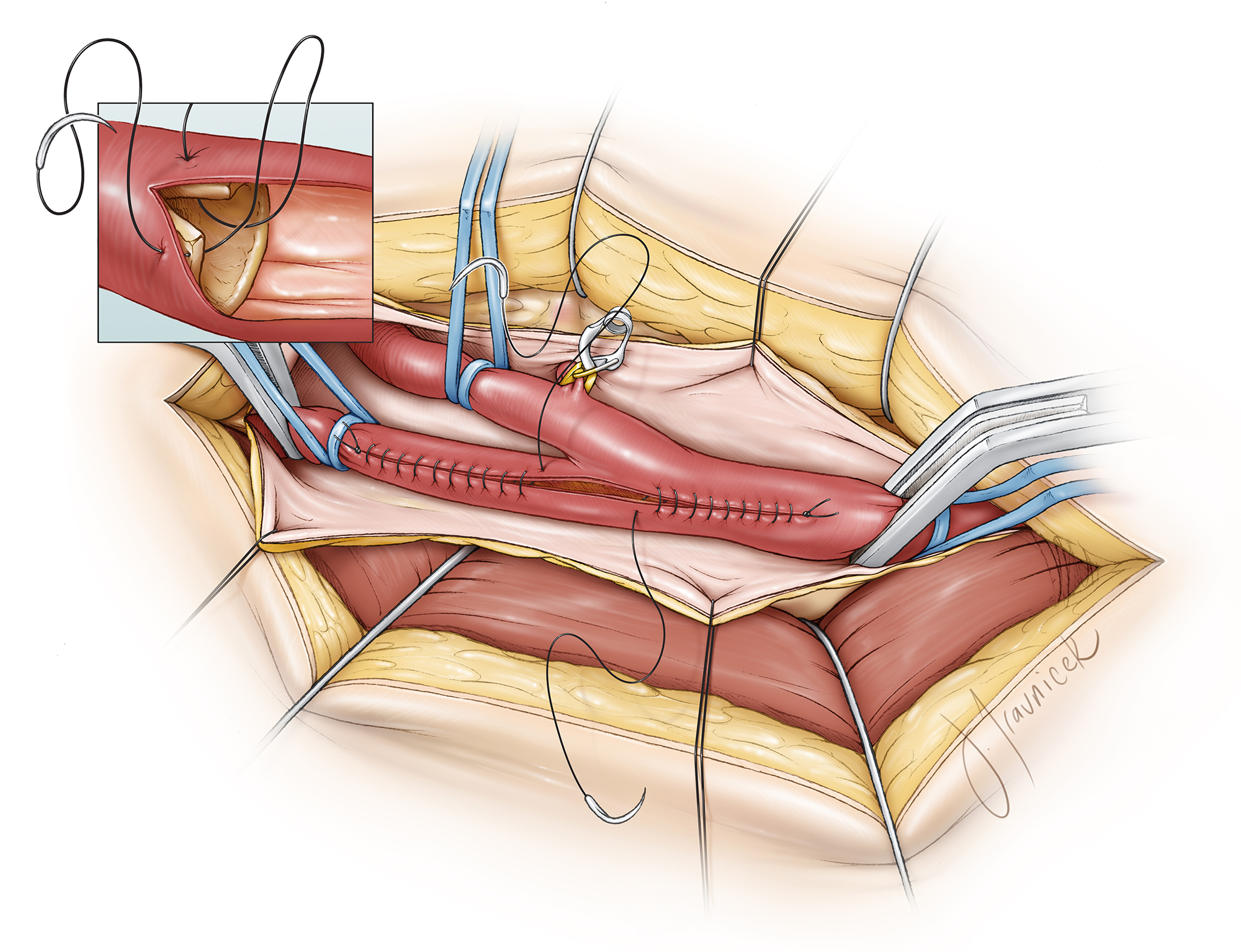
Figure 18: The arterial wall closure begins distally using a 6-0 prolene running suture. Front-wall intimal flaps should be included within the stitch to avoid arterial dissection. The suturing technique for the first few sutures along the ICA should be conducted with two passes of the needle (outside-in and inside-out, inset image). This maneuver ensures adequate tack-down of the intimal flaps and minimizes the risk of ICA constriction.
A second single-armed suture begins the closure at the proximal arteriotomy site using the same principles. This double-suture technique from both sides of the arteriotomy allows correction of wall-length discrepancies from either side, a feature especially helpful in cases where the arteriotomy is inadvertently not straight. Suturing can continue more efficiently in the middle section of the arteriotomy where the lumen is generous and larger bites of the wall can be incorporated into the closure without luminal constriction.
I pay special attention to include all arterial layers during suturing and to place the stitch in small enough intervals so that the chance of leakage is minimized. In addition, none of the adventitial tags are sewn into the lumen.
Periodic irrigation of the lumen with heparin solution continues during the entire process.

Figure 19: When the two stitches meet, prior to the final knot, the vascular loop or clip on the ICA is removed, allowing the artery to back-bleed twice, removing any debris or air that should not enter the distal cerebral circulation. The same maneuver is performed for CCA and ECA. The clamps are then reapplied and finally, the stitch is tied down (inset).
A heparinized saline syringe with a blunt tip is used to fill the lumen while the two stitches are held tight; I then lay down the knot. Next, the syringe is withdrawn, preventing air from entering the vessel.
Restoration of Circulation
The order of clamp removal is exactly opposite to the order of clamp placement just before the arteriotomy. First, the vessel loops/clamp on the ECA are loosened/removed, allowing any loose debris to be diverted toward the significantly collateralized arterial circulation of the face. The vascular clamp on the CCA is released next, restoring anterograde flow, again, into the ECA circulation.
At this point, there is often oozing from the arteriotomy suture line. Unless it is pulsatile in nature, it will almost always cease with time after tamponade treatment by a layer of SURGICEL or thrombin-soaked Gelfoam strips and intraluminal pressure reduction after restoration of the flow within the ICA.
Finally, the ICA circulation is restored with removal of the clamp or aneurysm clip prior to placement of additional sutures along the anastomosis line. Pulsatile bleeding, rather than oozing, is unlikely to stop and will require additional sutures. Gentle tamponade using a piece of gauze on the arteriotomy site typically stops the remaining ooze. EEG monitoring is continued for an additional 20 minutes after restoration of circulation.

Figure 20: The order of clamp removal and flow restoration is illustrated. This order of flow restoration is imperative to avoidance of distal embolization.

Figure 21: The details of shunt placement were reviewed in the above paragraphs. For placement of the shunt, the ICA is cannulated first, and the shunt is secured in place by pulling up on vessel loops; a mosquito clamp is used to hold the rubber sleeve in place. The shunt tubing is collapsed via heavy vascular forceps. The tubing is then cleared of air by briefly releasing the vascular forceps. Next, the distal end of the shunt is placed within the lumen of the CCA while the bulldog clamp on the CCA is removed. The shunt is then advanced into the CCA as the vessel loops or a custom clamp secures the shunt in place. To remove the shunt, I allow a small opening in the suture line of the lateral wall where the shunt can be extracted. I double clamp the shunt using mosquito clamps and then cut between the clamps. Each end of the transected shunt is then removed separately and the vascular clamps are reapplied.
Carotid Endarterectomy: Primary Closure of the Arteriotomy
Patch Angioplasty
The routine practice of patching the arteriotomy site is avoided. I selectively use a Hemashield patch when the ICA is of small caliber and the edges of the arteriotomy are uneven. The principles of suturing the patch are similar to those described above. The accompanying videos further illustrate the technique of patching.
The length of the patch material is tailored by placing the patch over the arteriotomy and cutting it to the appropriate length. The ends of the patch are then tapered. I use a double-armed 6-0 prolene suture to attach the ICA end of the patch to the distal end of the arteriotomy while rubber-shod clamps are used to hold the sutures in place. A running, nonlocking stitching method closes the medial wall from the ICA toward the CCA and continues to the midsection of the lateral wall. Next, the remaining lateral wall is sutured using the other arm of the double-armed suture.
With experience, CEA can be conducted in 2.5-3 hours with 30-40 minutes of cross-clamp time. Significant increase in this cross-clamp time is associated with an increased risk of cerebral ischemia.
The following intraoperative photos illustrate the operative steps for a right-sided endarterectomy:

Figure 22a: The skin incision (top) and the spreading action of the scissors for exposure of the carotid sheath (middle) are demonstrated. The common facial vein is isolated and two sutures will ligate the vein.

Figure 22b: The lateral side of the plaque is separated from the lumen of the carotid artery. Note the synergistic movements of the assistant and the operator.

Figure 22c: Similarly, the medial wall of the plaque is mobilized in expectation of its disconnection along its ends within the ICA and CCA. The extension of the plaque into the ECA is also separated.

Figure 22d: The plaque has been removed and the ICA lumen is carefully inspected. The plaque feathers down but a small shelf of intima may have to be tacked down during the closure of the arteriotomy.

Figure 22e: The lumen is carefully inspected and all the obvious free intimal flaps are removed.

Figure 22f: The small caliber of the ICA indicates the need for patch angioplasty. The needle is turned during its passage within the graft and the vessel walls to prevent leakage later.
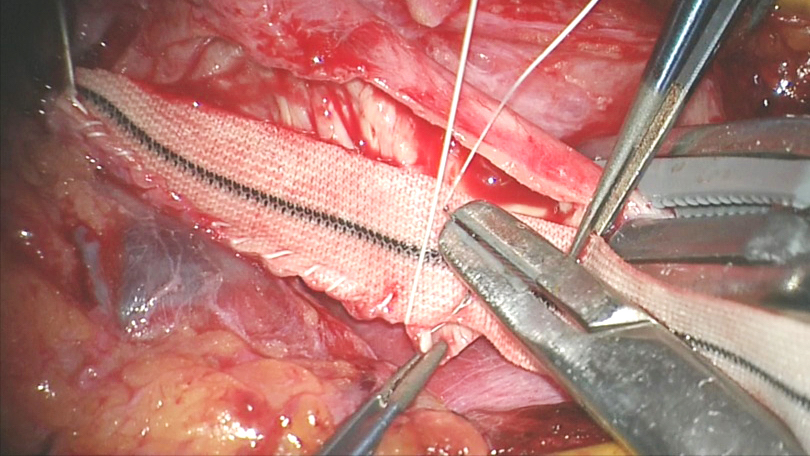
Figure 22g: Larger bites of the wall can be incorporated in the suture line to prevent the tags along the irregular edges from facing the lumen.

Figure 22h: The flaps along the proximal end of the arteriotomy in the CCA where the plaque was disconnected are tacked down using the suture.

Figure 22i: Similarly, the flaps along the distal end of the arteriotomy in the ICA are tacked down.

Figure 22j: The suture lines meet in the middle of the medial anastomotic line.

Figure 22k: The final result of patch angioplasty is demonstrated.
Closure
Adequate hemostasis is paramount. A small drain is left within the subplatysmal space. The drain will not prevent arterial bleeding from becoming symptomatic, but can potentially control slow venous ooze and serve as a warning sign (upon its sudden overflow) in case bleeding starts during the postoperative period. The drain should not provide the surgeon with a false sense of confidence, minimizing the importance of immaculate hemostasis. The drain is sutured in place and is removed during the first postoperative day.
The only layer closed underneath the skin and subcutaneous tissue is the platysma. This is completed with 3-0 vicryl sutures. The layers are approximated anatomically and not closed in a water-tight fashion. The deep dermis/subcutaneous tissues are also closed using 3-0 vicryl sutures. The skin is approximated using a 4-0 monocryl subcuticular suture.
The importance of a smooth wake-up with measures taken to avoid significant valsalva-like states (such as coughing) cannot be overestimated; this consideration must be requested from the anesthesia team.
Postoperative Considerations
Postoperative care consists of two important concepts. First, removal of the plaque often restores circulation that was previously absent. Higher degrees of preoperative stenosis correlate with increasing risks of postoperative intracranial hemorrhage due to hyperperfusion injury.
Postoperative blood pressure management is, therefore, paramount. Systolic blood pressure should not rise above 140 mmHg. This may require intermittent or continuous infusion of intravenous antihypertensive medications such as hydralazine or labetalol and/or initiation of oral medications.
Secondly, wound monitoring is important to detect the early stages of neck swelling because of hematoma accumulation. This is accomplished through visual inspection and palpation of the trachea. The drain output may also provide a clue.
A postoperative neck hematoma is most commonly from a venous source, but occasionally can be from an inadequate arteriotomy closure. The mass effect from the hematoma can obstruct the patient’s airway. The surgeon must be prepared to reopen the wound at the bedside to allow for decompression of the trachea, if necessary. This is an emergency and must be handled as such. Re-exploratory surgery often discloses nonspecific venous oozing from the deep tissues and bleeding from inadvertent puncture sites in the jugular vein.
Contributors: Casey Madura, MD , Ulas Cikla, MD, Mustafa K. Başkaya, MD
References
Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, Rankin RN, Clagett GP, Hachinski VC, Beckett DL, Thorpe KE, Meldrum HE, Spence JD. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1998;339:1415-1425.
Chambers BR, Donnan GA. Carotid endarterectomy for asymptomatic carotid stenosis. Cochrane Database Syst Rev. 2005:CD001923.
European Carotid Surgery Trialists' Collaborative Group. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: Final results of the MRC European Carotid Surgery Trial (ECST). Lancet 1998;351:1379-1387.
Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. Endarterectomy for asymptomatic carotid artery stenosis. JAMA. 1995;273:1421-1428.
Halliday A, Mansfield A, Marro J, et al. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet 2004;363:1491-1502.
Hobson RW 2nd, Weiss DG, Fields WS, et al. The Veterans Affairs Cooperative Study Group. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. N Engl J Med. 1993;328:221-227.
Rerkasem K, Rothwell PM. Carotid endarterectomy for symptomatic carotid stenosis. Cochrane Database Syst Rev. 2011:CD001081.
Related Materials
Other Atlases
Available Through the Atlas
-

Long-term prognosis and effect of endarterectomy in patients with...
-
Beneficial effect of carotid endarterectomy in symptomatic patien...
-
Hospital volume and surgical mortality in the United States
-
Benefit of Carotid Endarterectomy in Patients with Symptomatic Mo...
-
Protected carotid-artery stenting versus endarterectomy in high-r...
-
Guidelines for the early management of adults with ischemic strok...
-
Endarterectomy versus stenting in patients with symptomatic sever...
-
Guidelines for prevention of stroke in patients with ischemic str...
-
Efficacy of carotid endarterectomy for asymptomatic carotid steno...
-
Guidelines for the prevention of stroke in patients with stroke o...
-
Carotid artery stenting compared with endarterectomy in patients...
-
Immediate and late clinical outcomes of carotid artery stenting i...
-
The North American Symptomatic Carotid Endarterectomy Trial: Surg...
-
Early outcome of carotid angioplasty and stenting with and withou...
-
Long-term results of carotid stenting versus endarterectomy in hi...
-
Carotid artery stenting is associated with increased complication...
-
The causes and risk of stroke in patients with asymptomatic inter...
-
Guidelines for carotid endarterectomy: A multidisciplinary consen...
-
Carotid endarterectomy - An evidence-based review: Report of the...
-
Medical (nonsurgical) intervention alone is now best for preventi...
-
Carotid angioplasty and stenting versus carotid endarterectomy: R...
-
10-year stroke prevention after successful carotid endarterectomy...
-
Systematic review of the risks of carotid endarterectomy in relat...
Unavailable Through the Atlas
-
Endarterectomy for Asymptomatic Carotid Artery Stenosis
-
MRC European Carotid Surgery Trial: interim results for symptomat...
-
Randomised trial of endarterectomy for recently symptomatic carot...
-
Prevention of disabling and fatal strokes by successful carotid e...
-
Endovascular versus surgical treatment in patients with carotid s...
-
30 day results from the SPACE trial of stent-protected angioplast...
-
Analysis of pooled data from the randomised controlled trials of...
-
Endarterectomy for symptomatic carotid stenosis in relation to cl...
-
Carotid Endarterectomy and Prevention of Cerebral Ischemia in Sym...
-
Stenting in the carotid artery: Initial experience in 110 patient...
-
Results of the Stent-Protected Angioplasty versus Carotid Endarte...
-
Treatment and secondary prevention of stroke: Evidence, costs, an...
-
Early risk of recurrence by subtype of ischemic stroke in populat...
-
Endarterectomy Versus Angioplasty in Patients with Symptomatic Se...
-
Risk of stroke early after transient ischaemic attack: a systemat...
-
The appropriateness of carotid endarterectomy
-
Endarterectomy for moderate symptomatic carotid stenosis: Interim...
-
Results of a randomized controlled trial of carotid endarterectom...
Please login to post a comment.



