

Thalamic Tumors

Thalamic tumors are rare and comprise roughly 5% of all brain tumors.1 They occur in all age groups but are more common in children. In the past, risks of their resection were high given the deep-seated nature of thalamic tumors and the highly eloquent nature of the thalamic nuclei and fasciculi.
However, improvements in imaging modalities and microsurgical techniques have brought about new targeted cranial approaches that minimize surgical morbidity and maximize the safe extent of lesional resection. Therefore, as microsurgical techniques continue to progress, more effective surgical approaches to thalamic tumors have become achievable.2

ATLAS Choice Bipolar Forceps
Designed for your every surgical maneuver
Five tip sizes for brain and spine procedures
Unparalleled non-stick and low-profile features
CLINICAL PRESENTATION
Thalamic tumors have the potential to cause profound deficits due to disruptions in relay and integration of motor, sensory, and regulatory signals. Signs and symptoms are generally related to mass effect or disturbances of discrete thalamic nuclei. The former is the most common, resulting in symptoms related to increased intracranial pressure (ie, frontal headache, lethargy, and vomiting) and signs of papilledema.
The medial aspect of each thalamus forms the lateral borders of the third ventricle. Protrusion by way of tumor-inciting mass effect can cause noncommunicating hydrocephalus. Disruption of specific nuclei can elicit more specific findings. The following are specific divisions and their functional significance:
- Reticular and intralaminar nuclei: associated with arousal and pain regulation
- Sensory nuclei: regulate all sensory domains except olfaction
- Effector nuclei: govern motor language function
- Associative nuclei: connote cognitive functions
- Limbic nuclei: encompass mood and motivation
| Nucleus | Function |
| Sensory nuclei | |
| Ventroposterolateral (VPL) | Somatic sensation for contralateral body |
| Ventroposteromedial (VPM) | Somatic sensation for contralateral face, taste |
| Medial geniculate (MGN) | Hearing |
| Lateral geniculate (LGN) | Vision |
| Pulvinar | Visual processing |
| Motor nuclei | |
| Ventrolateral (VL) | Modulation and coordination of movement |
| Ventroanterior (VA) | Initiation and planning of movement |
| Ventrointermedial (VI) | Coordination of movement |
| Limbic and nonspecific projection nuclei | |
| Anterior (Ant) | Memory and storage |
| Mediodorsal (MD) | Motivation, drive, emotion |
| Centromedian (CM) | Emotional content of pain |
For example, invasion of the ventroanterior and ventrolateral nucleus can result in motor and coordination deficits due to projections to the cerebellum, basal ganglia, and supplementary motor cortex. Disruption of projections within the ventroposterolateral and ventroposteromedial nuclei can affect somatosensory relay from the body and face, respectively. Involvement of the pulvinar nuclei can cause changes in visual attention by way of altered communication with the visual cortex, whereas midline and intralaminar nucleus involvement can alter arousal stemming from associations with the hippocampus and reticular formation.2
EVALUATION
Magnetic resonance imaging (MRI) with contrast enhancement is the main diagnostic study of choice for these tumors. The use of contrast helps discern tumor from normal tissue. For glial tumors, contrast also provides an indication of histopathologic grade. It is important to glean vascular anatomy from T2-weighted MRI, taking note of the deep venous drainage because it is particularly important in posterior approaches.
The fluid-attenuated inversion recovery (FLAIR) sequence can be useful for tumors that do not enhance with contrast. A particular focus should be placed on the ventricular system to assess hydrocephalus. Diffusion tensor imaging (DTI) can help establish the relationship between the corticospinal pathway and thalamic tumors, especially the thalamopeduncular type. In these cases, preoperative DTI imaging is critical for selection of safe trajectory for tumor removal.

Figure 1: MR images of a thalamic pilocytic astrocytoma. This tumor was resected via a contralateral interhemispheric transcallosal approach.
PATHOLOGY
The vast majority of primary thalamic tumors are glial in origin.3 In adults, high-grade astrocytic tumors represent 40% of thalamic gliomas. Anaplastic astrocytomas and glioblastomas account for roughly 17% and 23% of these high-grade tumors, respectively. Less than 20% of all primary thalamic tumors are a germinoma, ganglioglioma, oligodendroglioma, dysembryoplastic neuroepithelial tumor, or neurocytoma.2
Thalamic tumors are often glial in nature and have been shown to contain p53, O-6-methylguanine-DNA methyltransferase (MGMT,) phosphatase and tensin homolog (PTEN), epidermal growth factor receptor (EGFR), and oligodendrocyte lineage transcription factor 2 (Oligo2) mutations. Histone H3-lysine 27-to-methionine (K27M) mutation has been used recently for the diagnosis of thalamic tumors linked to an entity known as diffuse midline glioma.2 Histone H3-K27M mutation is associated with aggressive disease and poor prognosis.4 Because this mutation is commonly found in the midline, the anatomic location of these tumors severely limits any opportunity for meaningful surgical resection, so treatment is limited to radiation and targeted chemotherapy.5
INDICATIONS
At present, no accepted standard guidelines exist for the specific treatment of tumors in the thalamic region.3 Most neurosurgeons adopt treatment guidelines that parallel histological equivalents in the lobar region. Those recommendations are maximal safe resection and chemoradiotherapy. Some surgeons elect to pursue diagnostic stereotactic needle biopsy followed by adjuvant therapy, depending on the diagnosis.2 Symptomatic hydrocephalus often requires surgical intervention for either placement of a ventriculoperitoneal shunt or surgical debulking to enable native cerebrospinal fluid (CSF) dynamics.
Recommendations exist for a number of specific tumor types. Pilocytic astrocytoma should be treated with maximal safe surgical resection because total or even near gross total resection can be curative. It is widely accepted that thalamic diffuse midline glioma, regardless of grade, is not a surgical disease because of its high rate of morbidity and death. I recommend adjuvant treatment for tumors that are consistent with a high-grade glioma on imaging and even avoid a biopsy as the biopsy can lead to symptomatic worsening in these patients with a short life span.
In contrast, radiologic features suggestive of low-grade glioma might warrant observation or resection if the tumor is approaching a pial surface. Biopsy is recommended for confirming diagnosis and molecular testing for guiding treatment.2,3 Radiosurgery can be used for small residual or recurrent tumors, for adjuvant treatment of higher-grade gliomas, and for palliation in patients unable to tolerate surgical resection.
As in the case of other tumors, the surgical candidacy of a tumor is significantly more likely with the tumor’s ability to approach a pial surface that is readily accessible, such as the posterior pulvinar and superior thalamus into the lateral ventricle.
PREOPERATIVE CONSIDERATIONS
Choosing the proper approach depends on the origin, growth pattern of the tumor in relation to normal structures and the suspected pathology. The surgeon’s level of comfort and experience with the chosen approach is also a significant driving factor. Numerous surgical approaches, including the anterior interhemispheric transcallosal, transcortical transventricular, contralateral infratentorial supracerebellar, posterior interhemispheric parasplenial, and transsylvian transinsular approaches, have been described.
Other considerations include the presence of hydrocephalus, the proximity of the tumor to critical neurovascular structures, and the location of important white matter structures (corticospinal tracts). Regardless of the approach, the surgeon should have a thorough understanding of the surgical, cortical and white matter anatomy that will be encountered and should pay particular attention to the vascular structures encountered in each approach.
OPERATIVE ANATOMY
The operative anatomy of the region is complex and is reviewed only briefly here.

Figure 2: The anatomy of the central core of the hemisphere. (A) Superior view. The central core is the part of the cerebrum located between the insula and the third and lateral ventricles. The upper part of the left hemisphere, except the precentral gyrus, has been removed to expose the frontal horn and body of the ventricle. The precentral gyrus is located lateral to the posterior part of the body of the ventricle and lateral to the splenium of the corpus callosum. The postcentral gyrus, which has been removed, faces the most anterior of the transverse temporal gyri, called Heschl’s gyrus. The short insular gyri are exposed anterior to and the long gyri behind the precentral gyrus. (B) Axial section extending through the central core crosses the anterior and posterior limb and genu of the internal capsule, the thalamus, and the lentiform and caudate nuclei at the level of the foramen of Monro. The lateral wall of the atrium and the roof of the temporal horn have been removed by dividing the white matter along the circular sulcus of the insula. (C) The posterior part of the lateral surface of the insula has been removed to expose the lateral surface of the lentiform nucleus. The choroid plexus is attached along the choroidal fissure that extends from the foramen of Monro to the inferior choroidal point located just behind the head of the hippocampus. (D) The anterior part of the insular cortex has been removed to expose the lentiform nucleus in the area above and behind the sylvian fissure, and above the anterior perforated substance and temporal horn. The middle cerebral artery, in the stem of the sylvian fissure, passes below the anterior part of the caudate and lentiform nuclei. The sublenticular and retrolenticular parts of the internal capsule, including the optic and auditory radiations, pass below and behind the lentiform nucleus. The anterior limb of the internal capsule is located between the caudate and lentiform nuclei, and the posterior limb is positioned between the lentiform nucleus and thalamus. (E) Enlarged view of the lower margin of the thalamus and upper part of the uncus. The anterior segment of the uncus contains the amygdala and faces the carotid and middle cerebral arteries. The posterior segment of the uncus contains the head of the hippocampus and is located anterior to the lower end of the choroidal fissure. The lateral geniculate body is located just above the choroidal fissure and body of the hippocampus. The choroidal fissure, along which the choroid plexus is attached, is located between the fimbria and the thalamus. The inferior choroidal point, the lower end of the choroidal fissure, is located behind the hippocampal head. (F) The thalamus has been removed and the fimbria of the fornix retracted laterally to expose the parahippocampal gyrus medial to the fimbria. The posterior cerebral artery courses through the crural and ambient cisterns on the medial side of the parahippocampal gyrus. The upper lip of the calcarine sulcus, formed by the cuneus, has been removed to expose the lower lip formed by the lingula. The deep end of the calcarine sulcus forms a prominence, the calcar avis, in the medial wall of the atrium. (Images courtesy of A L Rhoton, Jr.)
Venous Anatomy
An understanding of the parasagittal and deep diencephalic venous anatomy is important for executing many of the approaches. The venous anatomy and its variations around the superior parietal lobule should be noted before surgery for interhemispheric routes. Although the parasagittal veins are frequently sparse in this location, there are hemispheres in which the nondispensable duplicate forms of the vein of Trolard are present.
The deep veins such as the vein of Galen can complicate access via the supracerebellar approaches.

Figure 3: Veins in the roof of the third ventricle. (A) Superior view of the frontal horn and body. The thalamostriate and superior choroidal veins converge on the posterior edge of the foramen of Monro. The superior and anterior margin of the foramen of Monro is formed by the fornix. (B) The fornix has been folded backward to expose the tela choroidea and the internal cerebral veins in the roof of the third ventricle. A thin layer of ependyma extends above and partially hides the thalamostriate veins coursing along the sulcus between the thalamus and caudate nucleus. The anterior caudate and anterior septal veins cross the lateral and medial wall of the frontal horn. The posterior caudate veins cross the lateral wall of the body of the ventricle. Only a small part of the upper layer of tela located between the fornix and internal cerebral veins remains. (C) The internal cerebral veins have been separated to expose the branches of the medial posterior choroidal artery and the lower layer of tela choroidea that forms the floor of the velum interpositum in the roof of the third ventricle. The lower wall of the velum interpositum, in which the internal cerebral veins and medial posterior choroidal arteries course, is formed by the layer of tela attached along the medial side of the thalamus to the striae medullaris thalami. (D) The lower layer of tela has been opened and the internal cerebral veins and the medial posterior choroidal arteries have been retracted to expose the posterior commissure, pineal gland, and massa intermedia. (E) Another hemisphere. The upper part of the hemisphere has been removed to expose the frontal horn, body and atrium of the lateral ventricle. The choroid plexus is attached along the choroidal fissure. The anterior and posterior caudate veins cross the lateral wall and the anterior and posterior septal veins cross the medial wall of the frontal horn and body of the lateral ventricle. The superior choroidal veins course along the choroid plexus. The thalamostriate veins pass through the posterior margin of the foramen of Monro. The choroid plexus in the atrium expands to a large tuft called the glomus. (F) The body of the fornix has been removed to expose the internal cerebral veins coursing in the roof the third ventricle. The medial and lateral atrial and anterior calcarine veins join the posterior end of the internal cerebral veins. The basal veins are exposed below and lateral to the internal cerebral veins. (Images courtesy of A L Rhoton, Jr.)

Figure 4: Deep thalamic veins. (A) Posterosuperior view of the ventricles with the upper part of the cerebral hemisphere removed. The right occipital lobe and the adjacent tentorium have been removed to expose the upper surface of the cerebellum. Anterior caudate and anterior septal veins drain the walls of the frontal horn and empty into the anterior end of the internal cerebral vein. The posterior caudate veins drain the lateral wall of the body of the ventricle. (B) Enlarged view. The internal cerebral and basal veins converge on the vein of Galen. The lateral atrial vein crosses the pulvinar and empties into the internal cerebral vein. The anterior calcarine vein drains the depths of the calcarine sulcus and joins the vein of Galen near its junction with the basal vein. The calcarine sulcus forms a prominence, the calcar avis, in the medial wall of the atrium. The posterior end of the hippocampus is located at the anterior edge of the calcar avis. The veins exiting the ventricle pass through the margins of the choroidal fissure located between the fornix and thalamus. (C) The section of the left cerebrum has been extended forward into the temporal horn and hippocampus. The inferior ventricular vein drains the roof of the temporal horn and passes through the choroidal fissure to empty into the basal vein. The lateral atrial vein crosses the posterior surface of the pulvinar to empty into the internal cerebral vein. Only the stump of the basal vein remains. (D) Enlarged view of the inferior ventricular vein passing through the choroidal fissure located between the fimbria and lower surface of the pulvinar, to join the basal vein. The deep end of the collateral sulcus, located on the lateral margin of the parahippocampal gyrus, forms a prominence, the collateral eminence, in the floor of the temporal horn lateral to the hippocampus. (Images courtesy of A L Rhoton, Jr.)
The 6 Anatomical Thalamic Regions
It is very useful to divide the thalamus to 6 regions based on operative approaches to each region and their implications.

Figure 5: Operative regions for the anterior thalamus.

Figure 6: Operative regions for the posterior thalamus.
Region 1 (Anteroinferior)

Figure 7: The ventral anterior and inferior anterior nuclei of the thalamus are the primary nuclei in region 1. Region 1 is formed at its superior and medial borders by region 2 and at its posterior borders by region 3. The anterior and lateral portions of region 1 are defined by the edges of the genu and posterior limb of the internal capsule. The anterior perforated substance runs inferiorly to region 1, and it is immediately above the internal carotid artery bifurcation.6
Region 2 (Medial)

Figure 8: The nuclei in region 2 are the superior anterior nuclei, the medial nuclei, and the medial portion of the centromedian nuclei of the thalamus. Region 2 contains both thalamic (superior) and hypothalamic (inferior) structures that project into lateral and third ventricles. The anterior border of region 2 is shaped by the thalamostriate vein just behind the foramen of Monro. Medially, region 2 borders the superior choroidal vein, the choroid plexus, and the foramen of Monro. The lateral margin of region 2 is formed by the internal medullary lamina and Region 3. Inferiorly, region 2 is formed by the lateral wall of the third ventricle. The posterior wall of region 2 is shaped by region 4 and a small portion of the quadrigeminal cistern. Superiorly, region 2 is bordered by the lateral ventricle and the corpus callosum.6
Region 3 (Lateral)
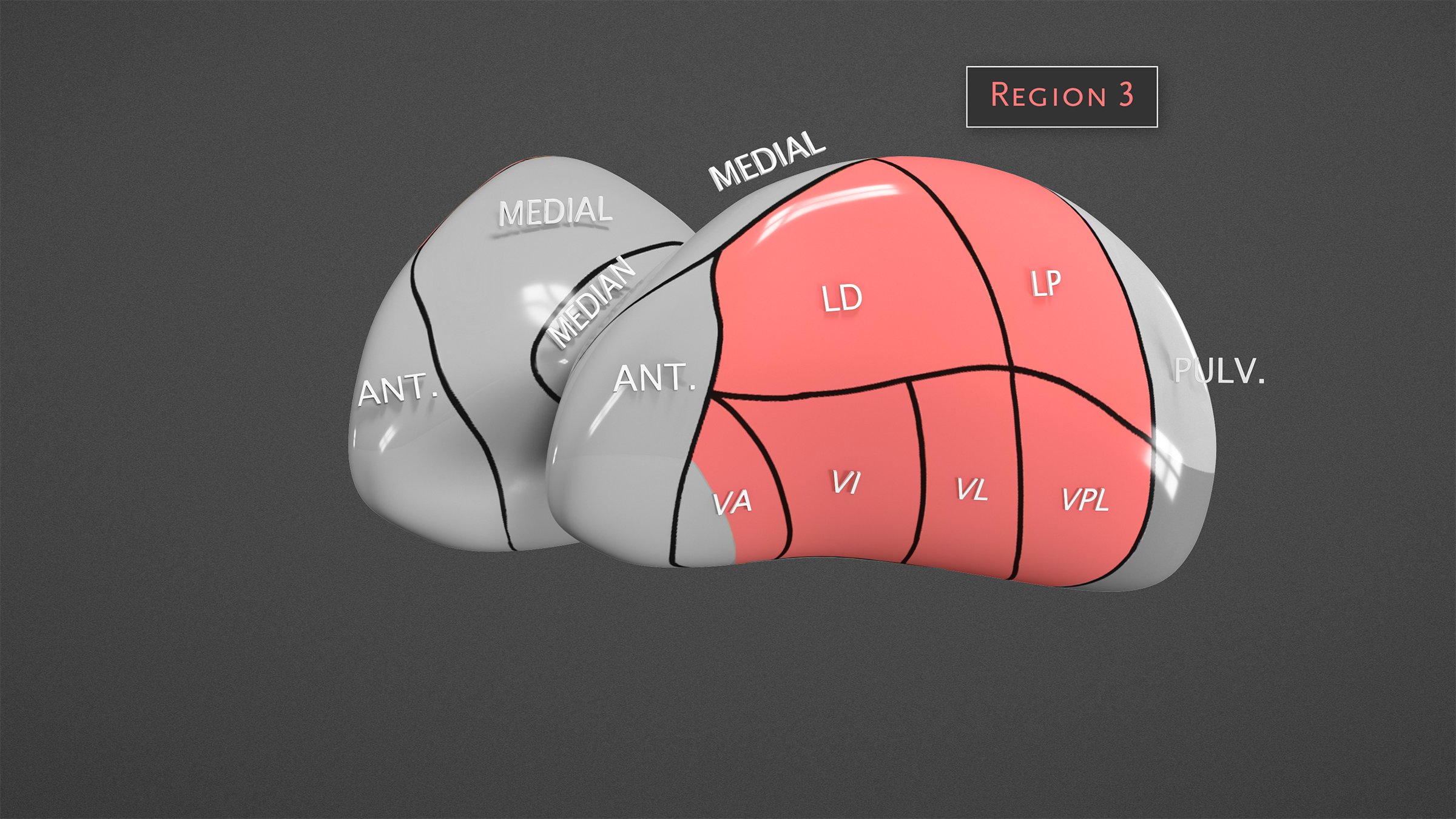
Figure 9: Region 3 contains the lateral nuclei which include the ventral anterior, ventral lateral, ventral posterior, lateral dorsal, and lateral posterior nuclei. The medial border of region 3 is formed by internal medullary lamina and region 2. The lateral border of region 3 consists of the genu and posterior limb of the internal capsule. Posteriorly, region 3 abuts the pulvinar (region 4). The anterior border is formed by region 1. Superiorly, region 3 is bordered by the caudate nucleus and lateral ventricle. Anteroinferior border is the hypothalamus, and the rest of the inferior portion is the cerebral peduncle.6
Region 4 (Posterosuperior)

Figure 10: Region 4 contains the pulvinar, the crus of the fornix, and the tail of the caudate nucleus. The anterior portion of region 4 is formed laterally by region 3 and medially by region 2. Superiorly, region 4 is bordered by the lateral ventricle and the corpus callosum. Its lateral border is shaped by the posterior limb of the internal capsule. The ambient and quadrigeminal cisterns make up the posteromedial margin. Region 6 (medial) and region 5 (lateral) define the inferior border of region 4. Region 4 is subdivided into 2 smaller regions divided by the choroidal fissure, where the lateral ventricular part represents region 4A and the medial cisternal part represents region 4B.6
Region 5 (Lateral Posteroinferior)

Figure 11: Region 5 is closely associated with the lateral geniculate body but contains no specific nuclei. The medial portion of region 5 is formed by region 6. Laterally, region 5 borders both the posterior limb of the internal capsule and caudate nucleus. It additionally projects laterally into the anterior wall the lateral ventricle. The inferior portion of region 5 is the midbrain. The ambient cistern makes up the posterior margin. The superior margin is formed by region 4, and the anterior margin is formed by region 3.6
Region 6 (Medial Posteroinferior)

Figure 12: Region 6 is closely associated with the medial geniculate body but contains no specific nuclei. Regions 2 (medial) and 3 (lateral) form the anterior border of region 6. The lateral portion of region 6 is shaped by region 5. The lateral habenular nucleus, habenular commissure, and pineal gland all reside medially to region 6 and are associated with its border. The inferior portion of region 6 is the midbrain. The quadrigeminal cistern makes up the posteromedial margin, and the superior margin is formed by Region 4.6
| Superior | Inferior | Medial | Lateral | Anterior | Posterior | |
| Region 1 | Region 2 | Anterior perforated substance | Region 2 | Genu, posterior limb of the internal capsule | Genu, posterior limb of the internal capsule | Region 3 |
| Region 2 | Lateral ventricle, the corpus callosum | Lateral wall of the third ventricle | Superior choroidal vein, the choroid plexus, the foramen of Monro | Internal medullary lamina, region 3 | Thalamostriate vein | Region 4 (pulvinar), the quadrigeminal cistern |
| Region 3 | Caudate nucleus, lateral ventricle | Hypothalamus, cerebral peduncle | Internal medullary lamina, Region 2 | Genu, posterior limb of the internal capsule | Region 1, hypothalamus | Region 4 (pulvinar) |
| Region 4 | Lateral ventricle, the corpus callosum | Region 6 (medial) and region 5 (lateral) | Ambient and quadrigeminal cisterns | Posterior limb of the internal capsule | Region 3 (lateral), region 2 (medial) | Ambient and quadrigeminal cisterns |
| Region 5 | Region 4 | Midbrain | Region 6 | Posterior limb of internal capsule, caudate nucleus, anterior wall the lateral ventricle | Region 3 | Ambient cistern |
| Region 6 | Region 4 | Midbrain | Lateral habenular nucleus, habenular commissure, pineal gland | Region 5 | Regions 2 (medial), 3 (lateral) | Quadrigeminal cistern |
RESECTION OF THALAMIC TUMORS
For approaches where early access to the CSF cisterns is not possible (ie interhemispheric and supracerebellar routes as compared to orbitozygomatic corridor,) intraoperative CSF drainage facilitates brain relaxation and expands the operative trajectory. This maneuver obviates the need for fixed retractors on the normal hemisphere. A lumbar drain is my method of choice for this purpose if deemed safe. Approximately 50 to 60 ml of CSF is removed gradually (in 10- to 15-ml aliquots) through the lumbar drain during craniotomy and after the dural opening.
For the interhemispheric routes, the patient is placed in the park-bench position with the normal unaffected hemisphere in the dependent position. This maneuver allows gravity retraction to mobilize the dependent (contralateral) hemisphere away from the midline. The patient is positioned with his or her neck tilted 45° upward away from the floor. However, positioning depends on the specific approach used and should be adjusted accordingly. Navigation is used for planning the incision and craniotomy to avoid veins and for designing the corticotomy.
Overall, I generally favor a contralateral interhemispheric approach over its ipsilateral counterpart when indicated, given that the former expands the lateral operative trajectory while minimizing the ipsilateral hemispheric retraction. The superior sagittal sinus and corresponding bridging veins over the superior parietal lobule should be evaluated with preoperative MRI, and if necessary, magnetic resonance venography (MRV) or computed tomography angiography (CTA) should be performed. The parasagittal bridging veins are often sparse in this region, but a risk of significant venous infarction exists with the ligation of any large vein.
Region 1: Anteroinferior Thalamic Tumors
Orbitozygomatic Transsylvian Supracarotid Infrafrontal Approach
This approach provides access to the anteroinferior thalamus. A very steep inferior-to-superior operative trajectory at the skull base is needed for this approach; therefore, an orbitozygomatic craniotomy with gentle depression of the orbital contents using dural retraction sutures is necessary.
After an orbitozygomatic craniotomy, performed in the posterior orbital region and anterior perforating substance, the dura is opened, and the sylvian fissure is dissected, exposing the olfactory nerve, supracarotid triangle, M1, and A1.
Next, a cortical incision is made from the lateral aspect of the olfactory nerve toward the posterior aspect of the medial orbital gyrus using navigation. The perforating arteries that supply the caudate nucleus, globus pallidus, putamen, anterior thalamus, and superior half of the internal capsule are identified and gently mobilized. It is critical to handle these vessels with care and bathe them in papaverine solution frequently to avoid their spasm. These vessels are very small caliber and are therefore very vulnerable. Their injury results in internal capsule stroke and represents the major risk of this operation. Note that the lenticulostriate arteries arising from the nearby A1 and M1 branches enter the anterior perforating substance in this territory and must be meticulously preserved.
The resultant surgical corridor is deepened further to reach the anteroinferior thalamus. For this approach, the uncinate fascicle, diagonal band of Broca, substantia innominata, and anterior commissure must be severed after cortical incision.
For more information on and visual diagrams of this approach, see the Orbitozygomatic Craniotomy chapter.

Figure 13: The steep inferior-to-superior trajectory mandates an orbitozygomatic route to the anterior inferior thalamus.
Transrostral/Subfrontal Translamina Terminalis Approach
This approach is preferred for accessing lesions of the medial anteroinferior thalamus. After supraorbital craniotomy with orbital rim osteotomy and dural exposure with the patient in the supine position, the interhemispheric fissure is opened gently. The rostrum, lamina terminalis, bilateral A1s, perforating arteries, and anterior communicating artery can be seen.
Through the transrostral route, an incision along the lamina terminalis initially exposes the massa intermedia and the third ventricle. The anterior commissure can be identified at the anteroinferior margin of the postcommissural fornix, and the medial anteroinferior thalamus is reached just posterior to the foramen of Monro in the vicinity of the most anterior part of the choroidal plexus. In this approach, resection of the rostrum leads to injury upon callosal fibers. For a wider exposure along the third ventricle, the surgeon can resect the anterior commissure after opening the lamina terminalis.7
This approach is limited to rather small anteroinferior thalamic tumors. Gross-total resection of large tumors is usually problematic and not feasible without undue retraction on the surrounding normal neurovascular structures. I am not in favor of this approach and prefer the orbitozygomatic route discussed above.
For more information on and visual diagrams of this approach, see the Subfrontal Translamina Terminalis Approach chapter.
Region 2: Medial Thalamic Tumors
Anterior Interhemispheric Transcallosal Approach
I prefer the contralateral anterior interhemispheric transcallosal approach for cases where the tumor epicenter is located at the anterior and medial thalamic region, reaching the pial surface into the wall of third ventricle. The cross-court contralateral route provides an excellent face-on view of the lesion on the medial wall of the third ventricle.
A craniotomy, measuring one-third behind and two-thirds in front of the coronal suture, is created. The medial extension of the craniotomy is placed over the superior sagittal sinus. The dura mater is opened in a horseshoe fashion with the base toward the superior sagittal sinus and reflected toward the sinus. Care should be taken to avoid injury to the cortical bridge veins. The bridging veins are preserved and untethered to increase the working zone through the interhemispheric corridor.
Two retention sutures are placed into the superior aspect of the falx to facilitate gentle dural sinus retraction and mobilization away from the midline. This maneuver is pertinent in expanding the interhemispheric corridor. A piece of Telfa pad is placed to cover and protect the normal hemisphere. The interhemispheric fissure is opened atraumatically under the microscope. Pericallosal arteries, callosomarginal arteries, and the anterior body of the corpus callosum should be exposed easily.
A 2-cm callosotomy is performed as guided by navigation. After the body of the lateral ventricle is accessed, several structures, including the fornix, choroidal fissure, lateral ventricular part of the medial thalamus, and caudate nucleus, are exposed. The foramen of Monro is enlarged using the transcallosal expanded transforaminal transvenous transchoroidal route. After the anterior choroidal fissure is opened, the part of the medial thalamus forming the lateral wall of the third ventricle and internal cerebral veins become visible. I leave the choroid plexus on the forniceal side during anterior transchoroidal dissection to protect the fornices. This contrasts with most other surgeons who believe to leave the plexus on the thalamic side. Protection of the fornices is of utmost importance due to the critical function of fornices in memory.
Postoperative transient mental disorders or memory deficits can occur in some cases. In addition, when the midcallosal fibers are severed, temporary speech irregularities can occur.
For more information, see the Introduction to Third Ventricular Tumors chapter.

Figure 14: Operative corridor for the contralateral transcallosal expanded transforaminal transvenous transchoroidal route to the medial anterior thalamus.
Suprapineal Recess/Supracerebellar Transventricular Approach
This approach provides surgical access to the posterior third ventricular part of the thalamus through the suprapineal recess. A standard midline suboccipital supracerebellar craniotomy or contralateral paramedian supracerebellar approach is performed. Through this small corridor, the quadrigeminal cistern is opened by advancing on the cerebellar tentorial surface. The pineal gland, the vein of Galen, the basal vein, and the internal cerebral and internal occipital veins can be seen.
After both the medial posteroinferior (region 6) and the cisternal (region 4) part of the thalamus are exposed, the third ventricular part of the medial thalamus can be accessed between the pineal gland inferiorly and the vein of Galen. After the third ventricle is entered, the aqueduct can be exposed in the base, whereas the third ventricular part of the medial thalamus can be reached laterally.
The disadvantages of this approach include the vulnerability of the habenula, vein of Galen, and quadrigeminal plate. Most deficits related to manipulation are temporary. In addition, this surgical route is one of the few transcranial transcisternal interventions in which endoscopy is superior to a microsurgical technique. The exposure is very limited and the corridor is very long.
For more information on and visual diagrams of this approach, see the supracerebellar transventricular approach chapter.
Region 3: Lateral Thalamic Tumors
Contralateral Anterior Interhemispheric Transcallosal Approach
This approach allows the lateral part of the thalamus to be reached. The head is positioned in such a way that the lesion is in the nondependent thalamus and the craniotomy is performed contralateral to the lesion.
The details of dissection are described above. Of note, the contralateral lateral ventricle is entered after the callosotomy. As a result of the contralateral approach, a more feasible lateral cross-court trajectory is achieved toward the lateral thalamus. Care should be exercised during removal of lateral thalamic lesions because of the close adjacency of the internal capsule.

Figure 15: Use of the contralateral transcallosal route is favorable for superior and lateral thalamic tumors. The expanded advantages of the cross-court trajectory (green) over the ipsilateral corridor (blue) are apparent.

Figure 16: Dissection route for the contralateral transcallosal route.

Figure 17: Steps of tumor removal. The suction device provides countertraction to allow for dynamic tumor separation from the rest of the peritumoral area.
In necessary and for medially situated tumors approaching the medial wall of the third ventricle, the foramen of Monro is enlarged using the transcallosal expanded transforaminal transvenous transchoroidal route.

Figure 18: The more lateral anterior thalamic tumors are also approached via the contralateral transcallosal expanded transforaminal transvenous transchoroidal route
Region 4: Posterosuperior Thalamic Tumors
Posterior/Occipital Interhemispheric Transcallosal Approach
The posterior interhemispheric transcallosal approach is preferred for pulvinar lesions that reside primarily medially (within 1 cm from the lateral border to the midline) within the posterosuperior thalamus. After a parieto-occipital parasagittal craniotomy, following the line of the precuneus, the splenium of the corpus callosum is reached under the inferior sagittal sinus. Most of the splenium must be spared to prevent the risk of disconnection syndrome. In fact, the more attenuated part of the posterior callosum is preferably entered and the splenium is spared.
An anterior-to-posterior working angle is used to prevent the need to transect the splenium. Just below the level of the splenium, the pineal gland and the fusion of the internal cerebral vein and vein of Galen can be seen. After entry into the ventricle, the bulbus of the corpus callosum and calcar avis can be seen medially, whereas the lateral ventricular part of the pulvinar and the choroid plexus can be observed in the anterior wall of the atrium. After opening the choroidal fissure through the transchoroidal approach, the cisternal part of region 4 is reached medially.
Endoscopic visualization of the surgical field through the splenial aperture widens the area of surgical exploration. Disadvantages of this approach include splenial retraction and its possible resection leading to temporary disconnection syndrome.

Figure 19: Posterior/occipital interhemispheric transcallosal approach. Splenium callosotomy is kept to a minimum, and an anterior-to-posterior trajectory under the posterior callosotomy is used to access the lesion.
For more information on and visual diagrams of this approach, see the Posterior Interhemispheric Transcallosal Intervenous/Paravenous Variant chapter.
Parieto-Occipital Transventricular Approach
Occipital transventricular approaches can also be used for these tumors. Optic radiation injuries are the most common complication of this approach. The craniotomy spans the lambdoid suture, and can be altered based on navigation guidance and according to the position of the superficial bridging veins.

Figure 20: Parieto-occipital route to this area.
Posterior Interhemispheric Contralateral Transfalcine Transprecuneus Approach
This approach allows the posterosuperior part of the thalamus to be reached. The patient is placed in the park-bench position so that the parieto-occipital lobe is deflected from the falx via gravitational effect, entailing a lesser need for retraction. An understanding of the parasagittal venous anatomy is important for the execution of this approach. The incision is typically linear and just behind the parietal bossing. This interhemispheric operative corridor is typically situated between 2 important bridging veins.
After the interhemispheric fissure is opened, the lingula, cuneus, parieto-occipital sulcus, and precuneus are visualized. After a cortical incision in the precuneus as guided by navigation, deeper exploration permits access to the atrium. After entry into the atrium, the lateral ventricular part of region 4, choroidal plexus, stria terminalis, and the fornix should be visualized in the opposite wall. Opening of the choroidal fissure enables access to the cisternal part of region 4. The entry point to the atrium can be variable because of the presence of parasagittal veins. Specifically, the transprecuneus approach severs the forceps major and cingulum fibers on the medial side and the superior longitudinal fascicule at its origin. I stay within the boundaries of the precuneus during deep dissection on the thalamus because the upper part of the optic radiations extends into the lower cuneus.
For more information on and visual diagrams of this approach, see the Contralateral Interhemispheric Transfalcine Transprecuneus Approach chapter.
Superior Parietal Lobule Approach
The patient is positioned in the three-quarter prone position with the parietal region at the highest point within the field. The craniotomy extends over the superior parietal lobule; the craniotomy should not cross the midline. After the dura is cut and the precentral gyrus, central sulcus, postcentral gyrus, and superior parietal lobule are exposed, a cortical incision is made 1 cm posterior to the postcentral gyrus, and the incision can be extended up to the parieto-occipital sulcus. Navigation guides all above maneuvers.
This approach allows access to the body of the atrium and its junction with the lateral ventricle. Dissection proceeds along the intraparietal sulcus; a cortical incision can also be conducted to arrive more laterally on the atrium of the lateral ventricle. Within the ventricle, the calcar avis and bulbar projection of the corpus callosum can be seen in the medial wall of the atrium, whereas the collateral trigone can be seen laterally at the base; the choroid plexus, stria terminalis, and lateral ventricular part of the pulvinar can be identified in the anterior wall of region 4.
Opening the choroidal fissure allows access to region 4B. Using the superior parietal lobule approach can result in the severing of the superior longitudinal fasciculus, resulting in temporary speech impairments such as anarthria and dysarthria. The arcuate fascicle and the uppermost part of the optic radiations can also be under threat depending on the position of the incision in relation to its distance to the superior border of the inferior parietal lobule. Please see the Parietal Craniotomy chapter for further details.
Video 1: Diffuse periatrial AVM treated via the superior parietal lobule approach.
Transsylvian Transinsular Approach
The transsylvian transinsular approach is used commonly for thalamic tumors with a close relationship to the insula. The lesions can potentially displace the posterior limb of the internal capsule and the basal ganglia anteriorly and therefore create an operative corridor via the postcentral insular sulcus. The patient’s head is rotated 15 to 20° away from the side of the lesion and extended 20°. This head position aligns the plane of the proximal sylvian fissure vertically, allowing the frontal and temporal lobes to fall naturally to either side as the fissure is split.
The approach consists of a pterional craniotomy and opening of the proximal part of the sylvian fissure. The dissection typically begins below the pars triangularis of the inferior frontal gyrus, where the distal sylvian fissure is widest. A cortical incision is made at this point, and the resultant surgical corridor is deepened to reach the posterior body of the lateral ventricle and atrium. Navigation guides various steps of subcortical dissection and preoperative tractography further confirms the safety of the route.
Disadvantages of this approach are that it may require the surgeon to sever the arcuate fasciculus, middle longitudinal fascicle, posterior part of the claustrocortical fibers and corona radiata, retrolenticular part of the internal capsule, and tapetum. The upper one-third of the optic radiations, tail of the caudate nucleus, and stria terminalis are in danger through the surgical corridor.
Video 2: Resection of a posterior insular lesion.
Region 5: Lateral Posteroinferior Thalamic Tumors
Subtemporal Transventricular Transchoroidal Fissure Approach
The lateral posteroinferior aspect of the thalamus can be accessed via this approach, which is particularly advantageous in reaching the thalamomesencephalic junction and the lateral geniculate body. The patient is frequently placed in the supine position with the head tilted to ~20 degrees toward the floor for gravity retraction to mobilize the temporal lobe away from the middle fossa. A lumbar drain is used before the craniotomy.
After a subtemporal craniotomy, the dura is incised and temporal lobe is elevated. Then, the upper end of the lateral mesencephalic sulcus, extending toward the medial geniculate body, is visualized. This is an important landmark allowing access to the lateral geniculate body. Preservation of the vein of Labbe is essential. Removing part of the parahippocampus and the medial part of fusiform gyrus reaches the temporal horn and opening the choroidal fissure exposes the lateral geniculate body. The fibers of the cingulum and inferior longitudinal fascicle are disrupted, and the anterior curve of the optic radiations, which form the Meyer loop, running backward toward the inferior part of the calcarine fissure, along with the tapetum, are at risk just superolateral to the resection site of the fusiform gyrus.7
Paramedian Supracerebellar Transtentorial Approach
This approach enables access to the lateral posteroinferior thalamus and is my favorite route. Its ipsilateral and contralateral counterpart (in the case of more laterally located lesions) is the safest and most efficient approach to the region.

Figure 21: The paramedian supracerebellar transtentorial approach (top) and its contralateral counterpart (bottom), in the case of more laterally located lesions, are the least disruptive routes to the lateral and medial posteroinferior masses.
It is particularly useful for accessing the temporobasal and mesial temporal areas, providing good exposure, especially for lateral posteroinferior thalamic lesions. A suboccipital craniotomy is performed via a paramedian vertical linear incision halfway between the inion and the mastoid groove and extending one-third above and two-thirds below the transverse sinus.
After opening the posterior fossa and with a “T” incision within the tentorium, the parahippocampal gyrus, collateral sulcus, pineal gland, and the superior and inferior colliculi are visualized. The posterior limit of the parahippocampal gyrus may be resected. After resection, the pulvinar thalami, fornix, temporal horn, and choroidal plexus should be visible.
Occasionally, posterior thalamic and vermian tumors mimic primary pineal region masses and displace the diencephalic veins posteriorly; this configuration is a potential contraindication for use of the midline supracerebellar approach, however, the paramedian supracerebellar approach may be a reasonable route.
For more information, see the Paramedian Supracerebellar Transtentorial and the Paramedian Supracerebellar Approach chapters.
Region 6: Medial Posteroinferior Thalamic Tumors
Infratentorial Supracerebellar Approach
Contralateral infratentorial supracerebellar approach is most suitable for lesions located at the medial portion of the cisternal pulvinar or lesions in the medial posteroinferior aspect of the thalamus. There are several variations to this approach: median, paramedian, and lateral. The patient should undergo a suboccipital craniotomy specific to the variation selected. I prefer a contralateral paramedian suboccipital craniotomy. While advancing on the cerebellar tentorial surface, I make a linear tentorial incision ipsilateral to the target pulvinar lateral to the straight sinus.
Dissection is carried down into the quadrigeminal cistern. Important structures that are recognized while reaching the medial posteroinferior thalamus in this region are the branches of the superior cerebellar artery, P3 segment of the posterior choroidal artery, the vein of Galen, internal cerebral veins, internal occipital vein, basal vein, vein of cerebellomesencephalic fissure, pineal gland, and the fourth cranial nerve.
The caution for preservation of the deep veins cannot be overemphasized. The vein of Galen can be displaced caudally or posteriorly and therefore be at high risk during the exposure. Care must also be taken to avoid injury to the posteromedial choroidal artery. It is important to note that there is no to minimal white matter destruction in this approach; therefore, this is my favored route (see Figure 21).
For more information on and visual diagrams of this approach, see the Pineal Region Tumor (Infratentorial Supracerebellar Approach) chapter.
Supracerebellar Transventricular Approach
This approach can be very useful to obviate the need for more complex and invasive routes such as the transcallosal transchoroidal routes that will require significant choroidal and forniceal dissection for reaching the posterior third ventricle.
I have used this route in very rare cases when the tectum is intact. In these cases, I have entered along a vertical line between ipsilateral and contralateral superior and inferior colliculi through the intercolliculi fissure. Patients have suffered from temporary dysconjugate extraocular movements.
For more information please see the Supracerebellar Transventricular Approach chapter.
ADDITIONAL APPROACHES
Transcortical Transventricular Approach
The transcortical transventricular approach is reserved for very large masses that project into the cortex or masses associated with enlarged ventricles. Trajectories can be via the frontal lobe, the occipital lobe, or the temporal lobe or via a transparietal approach. The most commonly used trajectory is the transfrontal trajectory. Each of these trajectories is associated with its own set of possible regional complications.
Endoscopic Approaches
Finally, if diagnosis via tissue biopsy is required and/or complete resection is not an option, endoscopic surgery can be considered.
INTRADURAL PROCEDURE KEY POINTS
For specifically trans-sulcal approaches, surgical resection of tumors can be potentially enhanced with the use of a tubular retractor. A preselected tubular retractor can be used to open a sulcus to its depth. It is passed to the superficial surface of the lesion with the aid of stereotactic navigation guidance. You can see an example case here. Tubular retractors should not be used for posterior fossa approaches.

Figure 22: Use of tubular retractors for ipsilateral removal of superior thalamic tumors. Enlarged ventricles are a favorable preexisting condition for this technique.
Pseudo en bloc resection is performed for thalamic tumors. The resection technique involves internal debulking with the use of a combination of tumor forceps, suction, tissue-biting pituitary rongeurs, ultrasonic aspirator, and/or bipolar cautery, followed by delivering the capsule of the tumor circumferentially in one piece. For cavernous malformations, the gliotic margins is left behind for avoid neurological morbidity.
CLOSURE
Once hemostasis is achieved, a ventricular catheter is implanted to drain debris within the ventricle and decrease the risk of hydrocephalus. If the surgical procedure was pristine, the drain may not be necessary.
POSTOPERATIVE CONSIDERATIONS
Patients are observed in the intensive care unit for 1 or 2 days before they are transferred to the general ward (for more postoperative care details, please see the Principles of Intraventricular Surgery chapter). Hypertension and overmedication with narcotics must be avoided. The ventriculostomy catheter is usually removed on the second postoperative day.
Postoperative MRI is obtained within 48 hours. Significant intraventricular work is associated with slow wake-up and the need for rehabilitation. If the patient has not been suffering from preoperative seizures, the prophylactic antiepileptics meds that were instituted at the time of surgery will be only administered for 1 week postoperatively.
PEARLS AND PITFALLS
- The ventricular walls are eloquent and should be respected. The least invasive route is the best route considering all the critical deep structures within the periventricular space.
- The approaches described within this chapter emphasize the importance of the operative working angles over the operative space for accessing these difficult-to-reach tumors.
Contributor: Andrew Witten, MD
References
- Cao L, Li C, Zhang Y, et al. Surgical resection of unilateral thalamic tumors in adults: approaches and outcomes. BMC Neurol 2015;15:229. doi.org/10.1186/s12883-015-0487-x
- Moses ZB, Friedman GN, Abd-El-Barr MM, et al. Tumors of the thalamus. In Spetzler RF, Kalani MYS, Lawton MT, eds, Surgery of the Brainstem. Thieme; 2020. doi.org/10.1055/b-0039-173906
- Ajlan A, Recht L. Neuro-oncologic considerations for pineal, thalamic, and brainstem tumors. In Spetzler RF, Kalani MYS, Lawton MT, eds, Surgery of the Brainstem. Thieme; 2020. doi.org/10.1055/b-0039-173913
- Solomon DA, Wood MD, Tihan T, et al. Diffuse midline gliomas with histone H3-K27M mutation: a series of 47 cases assessing the spectrum of morphologic variation and associated genetic alterations. Brain Pathol 2016;26:569–580. doi.org/10.1111/bpa.12336
- Himes BT, Zhang L, Daniels DJ. Treatment strategies in diffuse midline gliomas with the H3K27M mutation: the role of convection-enhanced delivery in overcoming anatomic challenges. Front Oncol 2019;9:31. doi.org/10.3389/fonc.2019.00031
- Rangel-Castilla L, Spetzler RF. The 6 thalamic regions: surgical approaches to thalamic cavernous malformations, operative results, and clinical outcomes. J Neurosurg 2015;123:676–685. doi.org/10.3171/2014.11.Jns14381
- Baran O, Baydin S, Gungor A, et al. Surgical approaches to the thalamus in relation to the white matter tracts of the cerebrum. World Neurosurg 2019;128:e1048–e1086. doi.org/10.1016/j.wneu.2019.05.068
- Belykh E, Yağmurlu K, Lei T, et al. Quantitative anatomical comparison of the ipsilateral and contralateral interhemispheric transcallosal approaches to the lateral ventricle. J Neurosurg 2018;128:1492–1502. doi.org/10.3171/2017.1.Jns161338
- Eichberg DG, Buttrick SS, Sharaf JM, et al. Use of tubular retractor for resection of colloid cysts: single surgeon experience and review of the literature. Oper Neurosurg (Hagerstown) 2019;16:571–579. doi.org/10.1093/ons/opy249
- Gassie K, Alvarado-Estrada K, Bechtle P, Chaichana KL. Surgical management of deep-seated metastatic brain tumors using minimally invasive approaches. J Neurol Surg A Cent Eur Neurosurg 2019;80:198–204. doi.org/10.1055/s-0038-1676575
Please login to post a comment.




