

Pericallosal Artery Aneurysm



Pericallosal cerebral aneurysms arise from the anterior cerebral arteries (ACA) and its branches distal to the anterior communicating artery (ACoA) complex. Most arise from the branching point between the callosomarginal artery and the main ACA trunk.
In 1948, Sugar and Tinsley described this aneurysm subtype as a relatively rare entity comprising about 5% of all intracranial aneurysms with a slight preponderance in females. Most reports suggest an incidence ranging from 2-9%. Pericallosal artery aneurysms are frequently associated with aneurysms in other locations.
Ruptured pericallosal artery aneurysms frequently present with intraparenchymal hematomas because of their position in the interhemispheric fissure and frequent adherence of their dome to the surrounding pial surfaces.
The interhemispheric corridor also confers a relatively narrow operative space for access and promotes obscured pathoanatomy. During the early stages of subarachnoid hemorrhage (SAH,) the friable and edematous brain presents technical challenges that the surgeon must confront to manage these aneurysms.
Many pericallosal aneurysms rupture when they are relatively small and can cause significant morbidity. Their coincidence with other aneurysms often mandates a pterional craniotomy in addition to an interhemispheric craniotomy. Occlusive treatment of small unruptured pericallosal aneurysms (<7mm) is potentially justifiable in patients with an otherwise good prognosis.
Compared with other anterior circulation aneurysms, pericallosal aneurysms are associated with a relatively higher risk of operative morbidity. Moreover, because of their rare occurrence and the increasing use of endovascular options, neurosurgeons have gained less experience with microsurgery of these specific aneurysms.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
Diagnosis
Ruptured pericallosal aneurysms present with signs and symptoms typical of aneurysmal SAH, but some special features should be noted. Radiographically, the hemorrhage appears more severe than seen with most other aneurysms.
Some patients may exhibit lower extremity monoparesis, paraparesis, or even hemiparesis, in association with a large medial intraparenchymal hematoma. A large intracallosal hemorrhage may result in hemispheric disconnection syndrome. There is a higher than usual incidence of poor clinical grades, with ~60% of patients presenting with Hunt-Hess grades of 3 or worse.
Evaluation
The standard tenets for radiographic evaluation of cerebral aneurysms are unchanged for pericallosal aneurysms, with the small caveat that imaging datasets (CT angiogram) compatible with intraoperative navigation obviate the need to acquire such data in a separate step. Interhemispheric dissection can be challenging in ruptured cases, and navigation can guide the surgeon toward the aneurysm neck and therefore minimize trauma to the cingula.
Computed tomography (CT) findings for ruptured pericallosal aneurysms are comparable with those of ACoA aneurysms. However, the hematoma often displaces the callosum inferiorly rather than superiorly, as is often seen with ACoA aneurysms.
The high resolution of catheter angiography remains the gold standard for evaluation of the aneurysm morphology, the finer details of neck geometry, and relationship to the parent vessels. These anatomic details are particularly important when considering the options between endovascular therapy and microsurgical clip ligation.
The laterality of the aneurysm should be noted, in particular, when both distal ACAs are opacified from ipsilateral injection because of a patent ACoA or a dominant A1 configuration of the ACoA complex.
Three-dimensional (3D) rotational angiogram allows me to manipulate the resulting image set interactively and trace out meandering and overlapping vessels. These sequences are especially important for defining the pericallosal aneurysm’s neck because CT angiograms, unlike for most other aneurysms, are frequently less effective in elucidating the neck morphology. I have a low threshold to obtain a catheter angiogram for pericallosal aneurysms.
Aneurysms smaller than 2 mm cannot be reliably detected on magnetic resonance angiography (MRA) or computed tomography angiography (CTA). I consider MRA data the least helpful for surgical planning. Callosal hemorrhages may mimic a glioma on delayed imaging (>1 week after hemorrhage). Moreover, calcified incidental pericallosal aneurysms may be confused with meningiomas.

Figure 1: CTA and 3D reconstruction arteriogram sequences demonstrate typical pericallosal aneurysms.
Isolated spontaneous intracerebral hematoma along the anterior parahemispheric region without SAH requires dedicated vascular imaging to rule out a vascular pathology in the area.
Indications for the Procedure
My preferences for clip ligation versus endovascular embolization of aneurysms are reviewed in the chapter titled Clip or Coil.
Pericallosal aneurysms often incorporate the origins of their afferent and efferent vessels and some are most suited for microsurgical clip ligation.
Clipping of calcified and sclerotic aneurysms may cause stenosis of or flow alterations within the pericallosal artery and subsequent distal ischemia that is difficult to predict with intraoperative imaging alone. These aneurysms should undergo endovascular intervention.
Preoperative Considerations
The need for a CT angiogram for intraoperative navigation and defining the location of the craniotomy and interhemispheric dissection was mentioned above. The parasagittal veins should be considered during operative planning for an interhemispheric craniotomy.
I prefer to have an external ventricular drain or a lumbar drain in place for the interhemispheric approach, especially during ruptured cases. This consideration is important because dominant cisterns are not accessible for cerebrospinal fluid (CSF) drainage, and brain tension can prevent atraumatic dissection between the cingula.
Operative Anatomy
The interhemispheric fissure and callosal cistern comprise a narrow space surrounded by the corpus callosum and bilateral cingulate gyri with intervening falx cerebri. The cingulate gyri can be densely apposed and adherent with interdigitating convolutions separated only by a very thin layer of arachnoid. Anterior parasagittal veins draining into the superior sagittal sinus can also restrict the approach. An associated frontal intracerebral or intraventricular hematoma may hinder optimal brain relaxation, and interhemispheric blood can obscure the normal anatomy.
The surgeon may find it challenging to obtain proximal vascular control because the distal pericallosal artery is commonly encountered before identification of the aneurysm and the proximal A2 segments hidden by the genu of the corpus callosum. The dome of the aneurysm may be densely fixed onto the cingulate gyrus. The aneurysm may also be located at the bifurcation of an unpaired azygos A2.
These technical challenges have to considered and managed appropriately.

Figure 2: The anterior cerebral artery (ACA) arises from the bifurcation of the internal carotid artery and courses rostromedially dorsal to the optic nerve as the A1 segment. The ipsilateral and contralateral A1 segments run together and connect via the ACoA. The pericallosal arteries are defined as the segments of the ACA distal to the ACoA. They continue superiorly into the interhemispheric fissure, upward on the medial surface of the hemisphere, and then course posteriorly on the superior surface of the corpus callosum, staying mostly below the lower margin of the falx (Image courtesy of AL Rhoton, Jr).
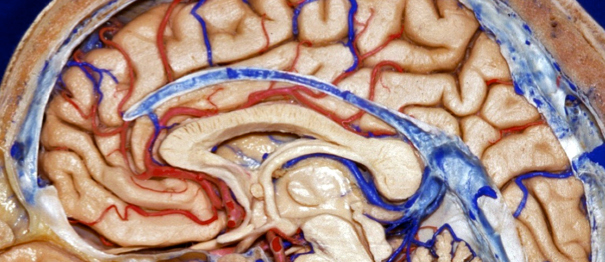
Click here to view the interactive module and related content for this image.
Figure 3: The pericallosal artery has the following segments, based on the preferred nomenclature by Perlmutter and Rhoton: A2 below the genu of the corpus callosum, A3 around the genu, and A4 and A5 as the terminal segments. Branches of the pericallosal artery can be divided into central and cortical groups: central perforators arise mostly from the A2 and A3 segments and enter the lamina terminalis and anterior forebrain below the corpus callosum to supply the anterior hypothalamus, septum pellucidum, medial portion of the anterior commissure, pillars of the fornix, and the anteroinferior parts of the striatum (Image courtesy of AL Rhoton, Jr).
The number of perforators is highly variable, an average of five arise from the A2 segment and three from each of the A3-A5 segments.
The eight cortical branches of the distal ACA include the orbital branches (orbitofrontal artery,) frontopolar artery, anterior, middle, and posterior internal frontal arteries, and paracentral, as well as superior and inferior parietal arteries. The callosomarginal artery is a major branch of the A3 segment. The pericallosal artery (A4 and A5) gives rise to the middle and posterior internal frontal and paracentral arteries.
The recurrent artery of Heubner can arise either from the A1 segment or the proximal A2 segment, and supplies the anterior medial part of the head of the caudate nucleus, adjacent parts of the internal capsule and putamen, and parts of the septal nuclei. The orbital branches supply the orbital and medial surfaces of the frontal lobe after arising from the ascending part of the distal ACA, ventral to the genu of the corpus callosum.
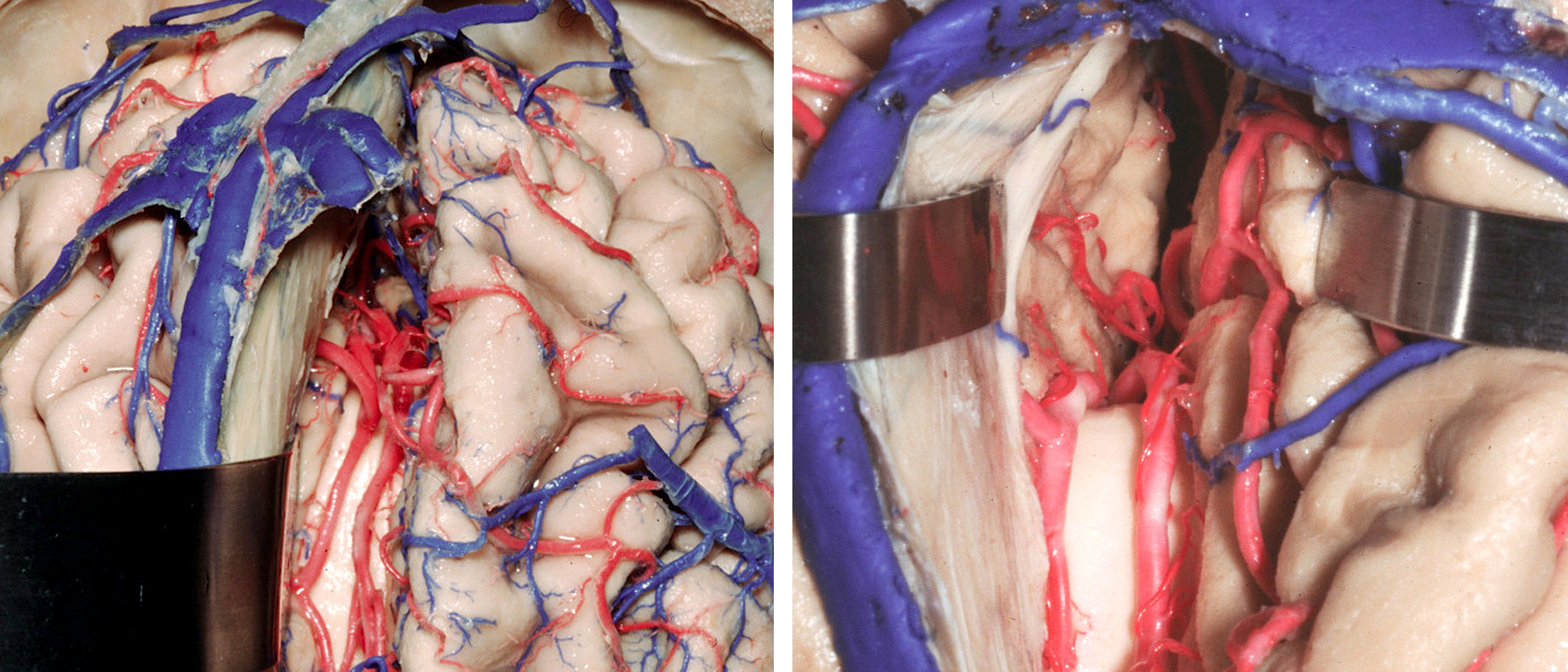
Figure 4: The callosomarginal artery is a major branch of the distal ACA, the most common location for pericallosal artery aneurysms, and its dissection guides the surgeon to the aneurysm. It arises distal to the frontopolar artery and the anterior internal frontal artery, and ascends dorsally within the callosomarginal sulcus. Branches of this artery supply the paracentral lobule and parts of the cingulate gyrus. This artery varies inversely in size with that of the distal pericallosal artery system and may be a distinct vessel or consist of a group of several ascending vessels that emerge individually from the pericallosal artery. The interhemispheric operative corridor is shown (Image courtesy of AL Rhoton, Jr).
The pericallosal artery, regarded as the terminal branch of the distal ACA, courses tightly along the corpus callosum on the medial surface of the parietal lobe, including the precuneus. Its collaterals include the dorsal callosal arteries arising from the posterior cerebral arteries that supply the splenium.
Anomalies and variations of the distal ACA are common. Both A2 segments usually arise from the respective ipsilateral A1 segments. A type I (azygos) variation includes a single A2 segment arising from the junction of both A1 segments, which then subsequently divides to supply both hemispheres. In the type II (bihemispheric) variation, one A2 is dominant and supplies significant portions of the contralateral hemisphere. The other A2 segment is hypoplastic and gives rise to only minor proximal branches.
An accessory (type III) variation features a small median third A2 segment that supplies some portion of either or both hemispheres. A careful study of an angiogram is warranted to understand these variations in configuration of the distal ACA complex and avoid confusion during surgery. Regardless of the proximal bifurcation anatomy, distal crossover vessels are relatively common, and although type I variations are rare, they are associated with pericallosal aneurysms in ~10% of individuals.
Aneurysms may occur anywhere along the course of the distal ACA, but are most common at its major branching points, including the genu of the corpus callosum and the origin of the callosomarginal artery.
Traumatic pseudoaneurysms frequently occur along the distal ACA segments adjacent to the free edge of the falx cerebri. These aneurysms are less likely to occur at branching points, and they may also occur along the proximal ascending portion of the callosomarginal artery.
The superficial cerebral veins arise from the cortex and subcortical white matter and form larger parasagittal veins, which empty into the dural sinuses. These larger veins include the superior (including the vein of Trolard) and inferior cerebral (Labbé) veins and the superficial middle cerebral (Sylvian) vein.
Click here to view the interactive module and related content for this image.
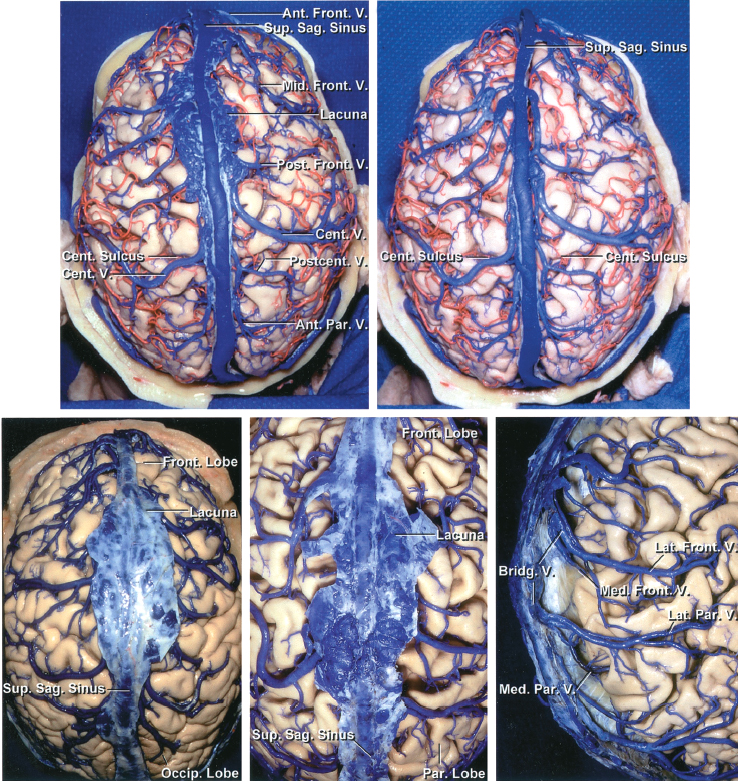
Figure 5: A variable number of parasagittal cerebral veins, usually 10 to 15, drain blood from the cortex and medial hemispheres and join the superior sagittal sinus. These veins enter the sinus by coursing obliquely forward after freely bridging a 1-2 cm gap between their most distal attachment to the pia-arachnoid and their entry into the sinus across the subdural space (Image courtesy of AL Rhoton, Jr).
Some of the parasagittal veins join a meningeal sinus (venous lake or lacuna) in the dura on their way to the superior sagittal sinus. The veins on the medial surface of the hemispheres drain into the inferior sagittal sinus.
MICROSURGICAL CLIP LIGATION OF PERICALLOSAL ARTERY ANEURYSMS
In general, a right-sided craniotomy is desirable for most pericallosal aneurysms because of the flexibility of brain mobilization over the inflexibility of the dura and falx retraction. This flexibility is more advantageous on the left side for a right-handed surgeon.
Although there is some merit to the approach from the nondominant side, the choice of the side must be counterbalanced by the anatomical considerations related to the location and direction of the dome and size of the aneurysm. If the aneurysm is covered by the falx, the contralateral approach requires a transfalcine route, which may not be desirable or easily avoided. I prefer to approach the aneurysm on the side away from its dome.
Some neurosurgeons argue that the horizontal position of the patient’s head is more ergonomic because the surgeon can then use both hands side-by-side rather than over the top.
If another aneurysm needs to be concurrently managed via a left pterional craniotomy, I prefer a small separate left parasagittal craniotomy through the same skin incision.
The location of the aneurysm dictates the optimal approach. I have found it useful to use three distinct approaches for aneurysms located on the A2 segment distal to the ACoA.
I prefer a pterional or orbitozygomatic approach for aneurysms near the ACoA complex. For rare aneurysms located more than 1 cm distal to the ACoA or ventral to the corpus callosum (infracallosal,) a basal frontal interhemispheric approach may be used. For aneurysms located above the genu or more distal (most common type,) I select the parasagittal interhemispheric corridor.

Figure 6: The typical location of a pericallosal aneurysm over the genu is shown. Securing proximal control via the interhemispheric route requires specific tenets. Resection of a small section of the genu is often necessary for this purpose.
There are a number of technical challenges that the interhemispheric, compared with the traditional pterional route, offers:
- A small and narrow operative corridor
- Management of the parasagittal veins
- A relatively small interhemispheric cistern and difficulty in achieving adequate brain relaxation early in dissection without compromising bridging veins and causing retraction injury
- The frequent dense adherence of the cingulate gyri to each other
In ruptured cases, the surgeon frequently encounters thick interhemispheric clot, causing operator’s disorientation about the appropriate operative trajectory and planes of dissection. This confusion can land the surgeon on the dome of the aneurysm without proximal control or lead to subpial transgression.
The surrounding vital vessels are generally highly adherent around the aneurysm neck and dome, requiring a flexible clipping strategy and thorough evaluation of the clipped aneurysm and parent vessels before finalizing the clip configuration. I frequently find myself repositioning the clip in these cases, and I often apply a “tentative clip” to gather the dome to be able to more effectively inspect the neck and prevent residual aneurysm and stenosed vessels.

Figure 7: Navigation guides the location of the incision and craniotomy (top images) for a typical pericallosal aneurysm reached via the interhemispheric route. A linear incision is adequate (second image). The lateral head position can take advantage of gravity retraction to mobilize the ipsilateral hemisphere. I use the supine head position (“nose up”) because I find this position more favorable for clip application. The placement of the burr holes/craniotomy (typically half way between the nasion and bregma) is outlined (third image) and the venous sinus is unroofed. Note the location of the retraction sutures in the superior aspect of the flax (bottom image) for mobilizing the sinus and expanding the interhemispheric corridor.
INTRADURAL PROCEDURE
For distal ACA aneurysms within 1 cm of the ACoA, I use a standard pterional craniotomy. I turn the patient’s head 15 to 30 degrees and position the malar eminence as the highest point in the operative field.
Using sharp microdissection, the A1 segment is identified and followed to the ACoA. Frequently, a small gyrus rectus resection is necessary to uncover the A2 segment and the aneurysm neck. Please refer to the Anterior Communicating Artery Aneurysm chapter for further details.
Initial Exposure
Infracallosal Aneurysms
For aneurysms arising more than 1 cm distal to the ACoA or near the genu, a basal frontal interhemispheric approach is used. The patient’s head is positioned in a neutral anatomic position. A bicoronal incision (more to the side of the craniotomy and just behind the hairline) allows harvest of a large pericranial graft to deal with the frontal sinus later, if necessary.
A unilateral parasagittal craniotomy that is guided by navigation exposes the midline. A small frontal sinus can be avoided by placing the craniotomy just above it, but sacrificing exposure is not a recommended trade-off. For exenteration of the frontal sinus, refer to the Bifrontal Craniotomy chapter.
Distal or Typical Pericallosal Aneurysms
Distal aneurysms are easier to deal with because their dissection is limited to the interhemispheric space. The patient’s neck is flexed 15-degrees and the head immobilized in the neutral position.
A direct interhemispheric approach with a craniotomy tailored to the location of the aneurysm based on navigation data is preferred. Navigation is helpful, but the craniotomy itself can be easily planned by studying a preoperative cross-sectional study that displays the aneurysm in a sagittal plane in relation to the coronal suture as a palpable landmark.
Next, A parasagittal frontal craniotomy (5-6cm in length) is conducted and the superior sagittal sinus is unroofed. Smaller craniotomies will limit the working angles and the surgeon’s ability to deal with unexpected parasagittal veins.
Microdissection to Secure Proximal Control
Infracallosal Aneurysms
A dural flap along the contours of the bone flap is raised and hinged on the superior sagittal sinus. The bridging veins are protected. A considerate choice must be made about sacrificing any vein to allow an adequate interhemispheric working zone.
A troublesome vein can frequently be dissected free of its encasing arachnoid without the need for its sacrifice. Image guidance can streamline the next steps in dissection, but if unavailable, the tenet of approaching the aneurysm from the side of the normal proximal arteries holds and allows proximal control. The closer the aneurysm is to the ACoA, the more imperative it is to begin dissection proximally and inferiorly.
Mobilization of the right hemisphere exposes the falx, which is followed to the crista galli. Next, the arachnoid adhesions between the hemispheres are further separated. Exposure of the suprachiasmatic cistern will reveal the ACoA complex and the A2 segments which lead me to the aneurysm.
It is paramount to resist the temptation to dissect directly toward the aneurysm and land on the dome. Minor adjustments in the operative trajectory lead to dramatic changes in the final reach of the corridor. The corpus callosum with its glistening yellow color can serve as a useful landmark. After proximal control is established, I gently dissect around the sides of the aneurysm. Partial resection of the callosum may be needed for safe exposure of the regional vessels and aneurysm neck.
Distal Pericallosal Aneurysms
Larger parasagittal veins are preserved. I have occasionally extended the craniotomy to the contralateral side and revised the side of approach upon finding indispensable large parasagittal veins ipsilaterally. The subdural space over the falx is entered and additional CSF is drained from the ventriculostomy catheter or lumbar drain to assist with brain mobilization.
Next, navigation can direct the location of intercingulate dissection just distal to the aneurysm neck. This step of dissection can be treacherous in the setting of SAH because the pial surfaces are inflamed and closely connected.

Figure 8: The callosomarginal artery is used as an interhemispheric landmark to find the corpus callosum and pericallosal arteries. The aneurysm is typically at the junction of the callosomarginal and pericallosal arteries and should be initially avoided. The last layer of transverse arachnoid bands often obscures the parallel pericallosal arteries situated over the callosum. If only one artery is apparent, the identity of the artery should be questioned and a wider exposure should be sought to expose both vessels.
If CSF drainage is desirable but no ventriculostomy or lumbar drain was installed, I complete a small callosotomy to relieve cranial tension.
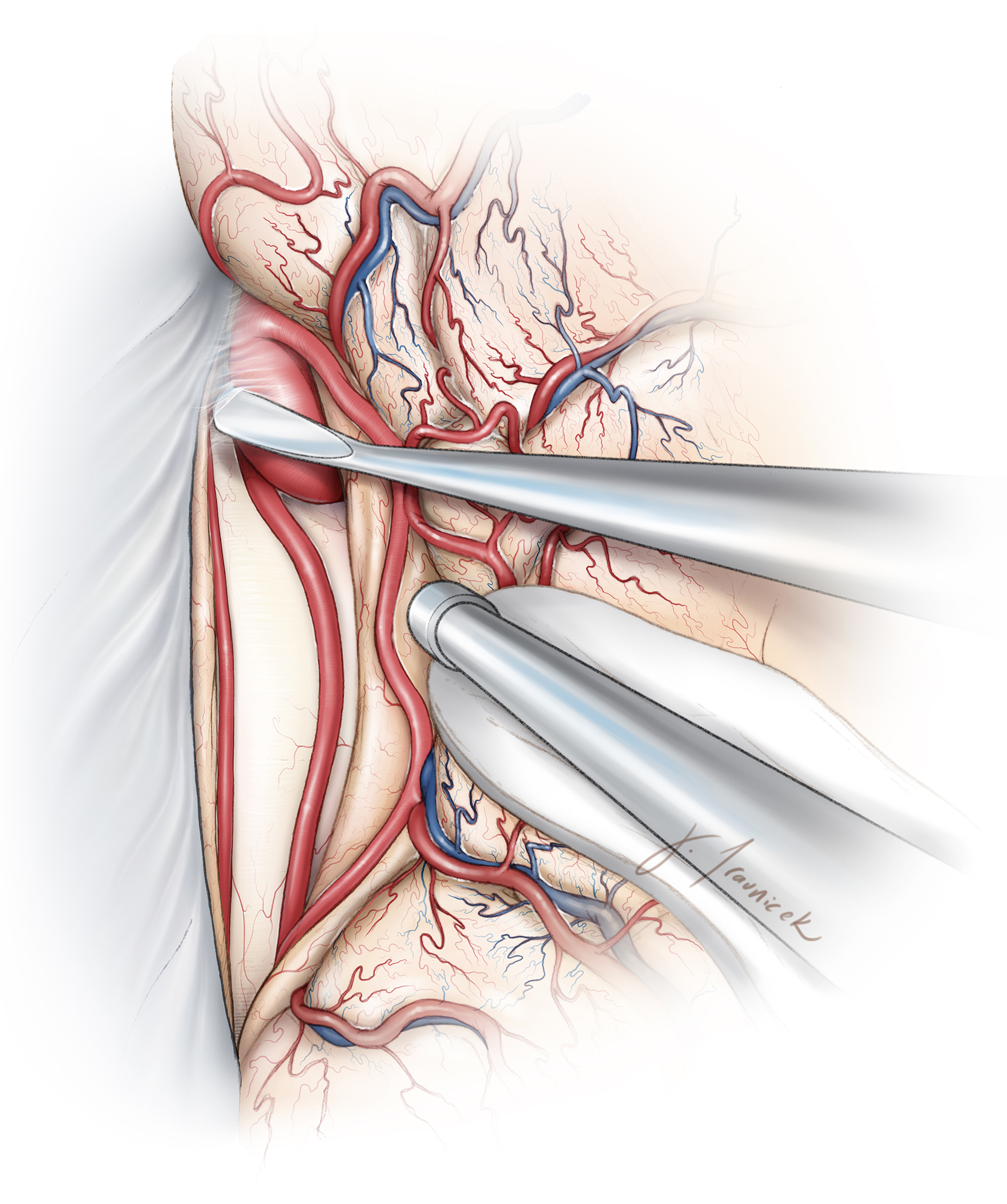
Figure 9: After the pericallosal arteries are identified, dissection proceeds anteriorly. It is important to stay close to the arteries and avoid wandering over the aneurysm dome. The dissection is pursued on the side of the aneurysm rather than directly on the dome. The projection of the aneurysm on preoperative imaging guides the operator to avoid the dome.

Figure 10: Once the aneurysm is barely visible and its location confirmed via navigation, a small portion of the genu just below the aneurysm is resected to allow exposure of the A2 branches anterior to the genu. These branches curve away from the instruments. This maneuver secures proximal control. The superior and anterior pial surfaces of the genu are dissected open.
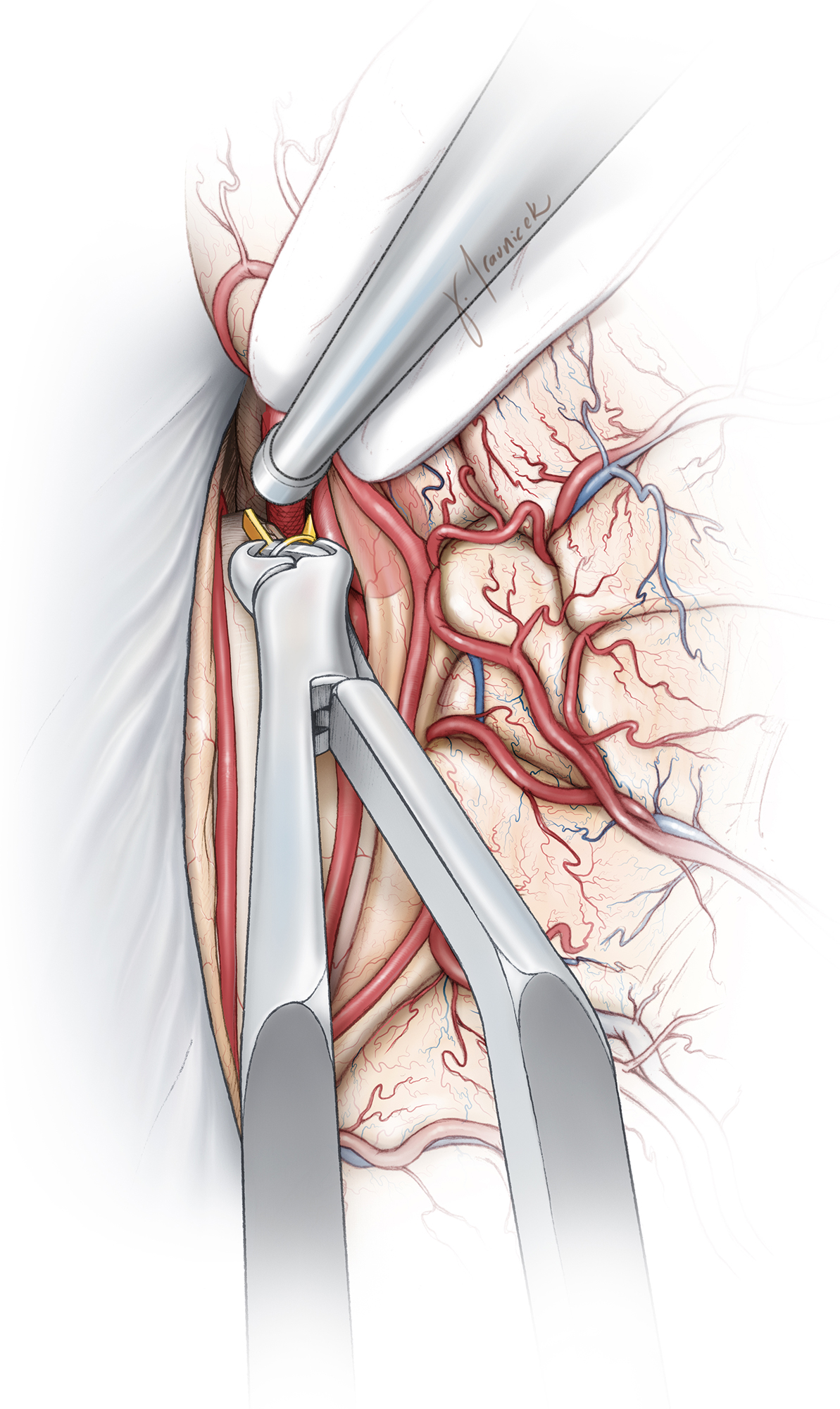
Figure 11: It is imperative to secure proximal control over the ipsilateral A2 before further dissection is contemplated around the neck. I leave the cortex overlying the aneurysm dome intact to avoid premature rupture. Aggressive retraction and manipulation of the surrounding tissues should be avoided to prevent such a rupture. The location of the dome should be kept in mind during subsequent operative maneuvers. Because vascular dissection is conducted in the retrograde distal-to-proximal direction, the lack of immediate proximal control can be unsettling to the surgeon.
In the case of an inadvertent intraoperative rupture, a small piece of cotton is placed over the bleeding dome and gentle pressure applied. This maneuver will control the bleeding without a need to resort to more radical measures, as the flow is not very brisk in the distal ACA territories. A retractor blade can hold the cotton in place while proximal control is secured.
Aneurysm Dissection and Clip Application
Infracallosal Aneurysms
Once the bilateral A2 branches have been identified, dissection for a temporary clip placement is pursued. I prefer to apply the permanent clip in line or parallel with the small caliber parent vessel to avoid its crimping and stenosis. This configuration also supports complete clip blade closure and avoids clip failure and slippage.
Clip application usually requires careful consideration of curved, fenestrated, or side-angled clips. After the clip is applied and the aneurysm punctured, the surgeon must complete a circumferential dissection and inspection around the aneurysm to ensure proper clip placement and exclude the risk of branch or perforator compromise.
Distal Pericallosal Aneurysms
The parent vessel must be identified both proximally and distally to obtain proximal control. These aneurysms often have a very complex neck configuration incorporating the proximal and distal small-caliber vessels. Temporary clip application allows thorough inspection of the neck while mobilizing the dome.

Figure 12: Temporary occlusion of ipsilateral A2 allows manipulation of the neck and dome so that the neck may be thoroughly studied. In addition, I use the tip of the suction device to gather the neck into the clip and achieve the desirable clip construct. Angled clips are often effective so that the clip appliers are not obstructing the operative view.
The manipulations of the vessels often lead to some degree of arterial spasm. Papaverine-soaked pieces of Gelfoam are used to cover these vessels temporarily to relieve their spasm.
Postoperative Considerations
The postoperative management of pericallosal aneurysms is similar to that of other cerebral aneurysms.
Pearls and Pitfalls
- Pericallosal aneurysms are approached in the distal-to-proximal direction along the distal ACA. Careful and strategic dissection is imperative to avoid rupture without proximal control.
- Cingula should be carefully protected and aggressive retraction on the medial hemispheres avoided. Injury to these regions can lead to substantial postoperative cognitive morbidity
Contributor: Clemens M. Schirmer, MD, PhD
References
Perlmutter D, Rhoton AL Jr. Microsurgical anatomy of the distal anterior cerebral artery. J Neurosurg. 1978;49(2):204-228.
Samson DM (ed): Intracranial Aneurysm Surgery: Techniques. Mount Kisco, NY: Future Publishing, 1990.
Related Materials
Available Through the Atlas
-

Microsurgical anatomy of the distal anterior cerebral artery
-
Saccular aneurysms of the distal anterior cerebral artery
-
Aneurysms of the pericallosal artery: a study of 14 cases verifie...
-
Treatment of anterior communicating artery aneurysms: Complementa...
-
Surgical strategy for distal anterior cerebral artery aneurysms:...
-
Microanatomy of the pericallosal arterial complex
-
Endovascular management of traumatic and iatrogenic aneurysms of...
-
Aneurysm of azygous anterior cerebral artery
-
Interhemispheric approach with callosal resection for distal ante...
Unavailable Through the Atlas
-

Multiple intracranial aneurysms in a defined population: Prospect...
-
The Cerebral Veins
-
Distal anterior cerebral artery aneurysms
-
Motor evoked potential monitoring during cerebral aneurysm surger...
-
Traumatic aneurysms of the pericallosal arteries
-
Aneurysms of the distal anterior cerebral artery and associated v...
-
Aneurysms of the pericallosal-callosomarginal junction
-
Incidence of berry aneurysms of the unpaired pericallosal artery:...
-
Pericallosal aneurysms
-
Distal anterior cerebral artery aneurysms: Treatment and outcome...
-
Anterior cerebral artery variations detected by MR angiography
-
Coiling of ruptured pericallosal artery aneurysms
-
Pitfalls in the use of spiral CT for identification of intracrani...
-
Brain resection for exposure of deep extracerebral and paraventri...
-
Aneurysms of the distal anterior cerebral artery: Results in 59 c...
-
Management of distal anterior cerebral artery aneurysms: A single...
-
Microneurosurgical management of aneurysms at the A2 segment of a...
-
Anatomic features of distal anterior cerebral artery aneurysms: A...
Please login to post a comment.




