

Toxoplasmosis

Toxoplasmosis is the most common opportunistic CNS infection associated with AIDS. When infecting the brain parenchyma, toxoplasmosis can cause a necrotizing encephalitis. It is caused by the parasite Toxoplasma gondii, whose oocytes are commonly found in the feces of birds and mammals, and domestic cats in particular.
Humans become infected when they ingest the oocytes, usually via uncooked and contaminated foods. The infection is often indolent, and most affected patients are asymptomatic. However, headache is the most common presenting symptom. Patients are at greatest risk of developing opportunistic infections when the CD4+ cell count falls below 200 cells/mm3.

ATLAS Choice Bipolar Forceps
Designed for your every surgical maneuver
Five tip sizes for brain and spine procedures
Unparalleled non-stick and low-profile features
Imaging Features
Toxoplasmosis usually presents as multiple parenchymal lesions with surrounding edema and central necrosis. However, the lesions may be few or solitary (only 14% were solitary in one study), and the morphology may be nodular or mass-like. The basal ganglia, thalamus and grey-white matter junction are the most commonly affected structures. The brainstem may also be involved.
Toxoplasmosis (and other infectious processes that cause microabscesses) should be considered in the differential diagnosis for multiple enhancing lesions.
- CT
- In the acute phase, CNS toxoplasmosis presents as multiple low-density lesions.
- In the chronic, post-treatment phase the lesions often calcify.
- MR
- T1-weighted images
- Hypointense lesions
- Often with ill-defined surrounding hypointense edema
- T2-weighted images
- Variable: iso- to hyperintense
- Lesions that develop into abscesses may appear centrally hyperintense (necrosis) with hypointense rim (capsule)
- Hyperintense signal surrounding the lesion due to edema
- FLAIR
- Perilesional hyperintensity reflecting edema
- DWI/ADC
- Lesion, capsule and/or cavity may demonstrate restricted diffusion (hyperintense on DWI and hypointense on ADC)
- GRE/SWI:
- Decreased signal (“blooming” artifact) compatible with hemorrhage may be seen, which can help to distinguish toxoplasmosis from lymphoma (3).
- T1 with Contrast: Variable
- Nodular or ring-enhancing
- Target-like enhancement of ring with eccentric mural nodule is highly specific for toxoplasmosis but is only seen one third of the time
- MR Spectroscopy
- Increased lactate and lipids
- Decreased NAA and Choline
- T1-weighted images
- Nuclear Medicine
- F-18 PET/CT: Lesions may take up tracer. F-18 PET cannot definitively distinguish toxoplasmosis from lymphoma or metastases.
- Thallium SPECT: Lack of uptake in toxoplasmosis (avid uptake in lymphoma/metastases).

Figure 1: Non-contrast CT demonstrates multiple isodense lesions with surrounding hypodense perilesional edema.
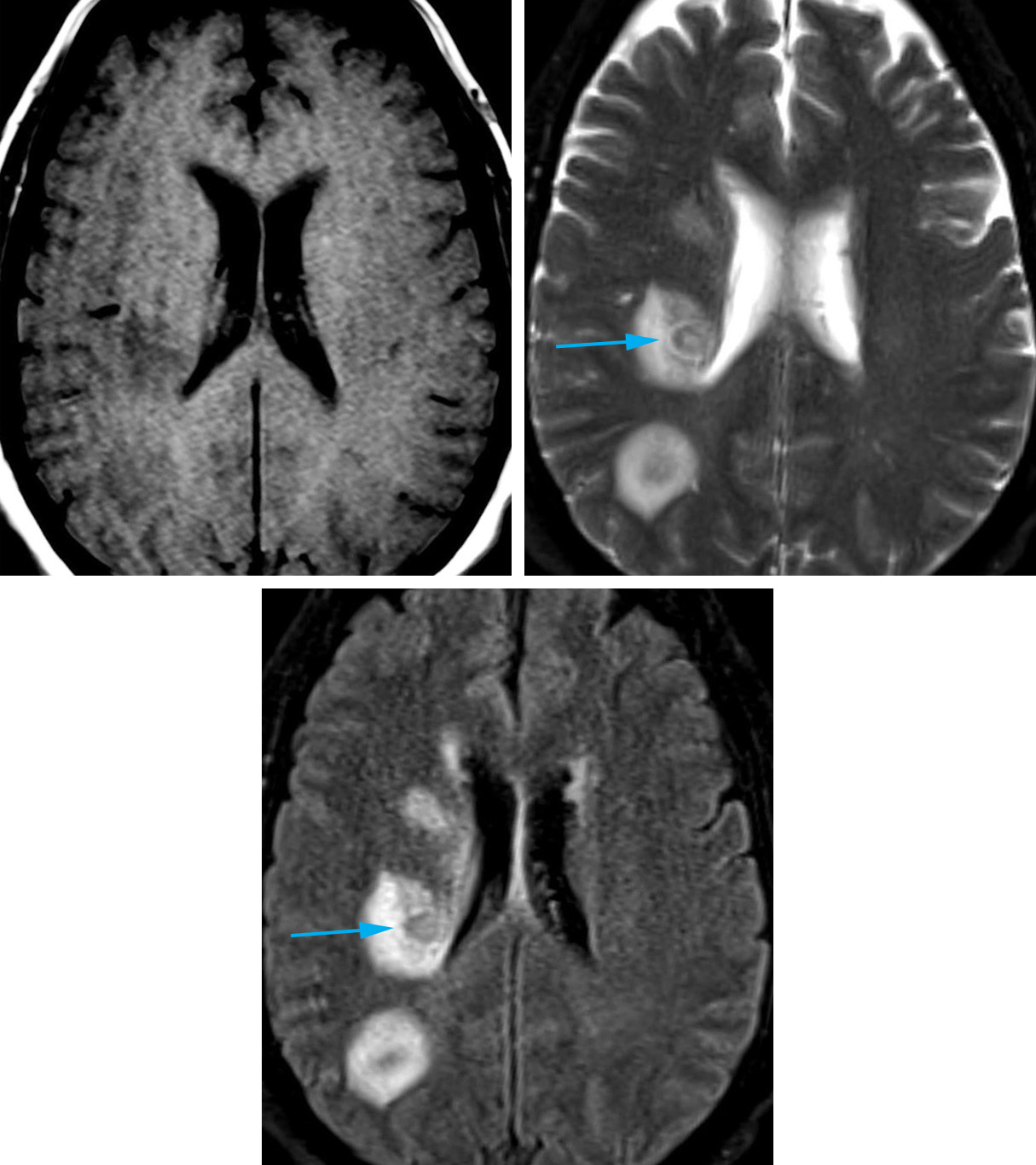
Figure 2: T1 – hypointense anterior lesion, isointense posterior lesion (top row left). T2 and FLAIR – Perilesional bright signal reflecting vasogenic edema (top row right). A discrete capsule with dual hyperintense and hypointense rim is sometimes visible (bottom row, arrows).
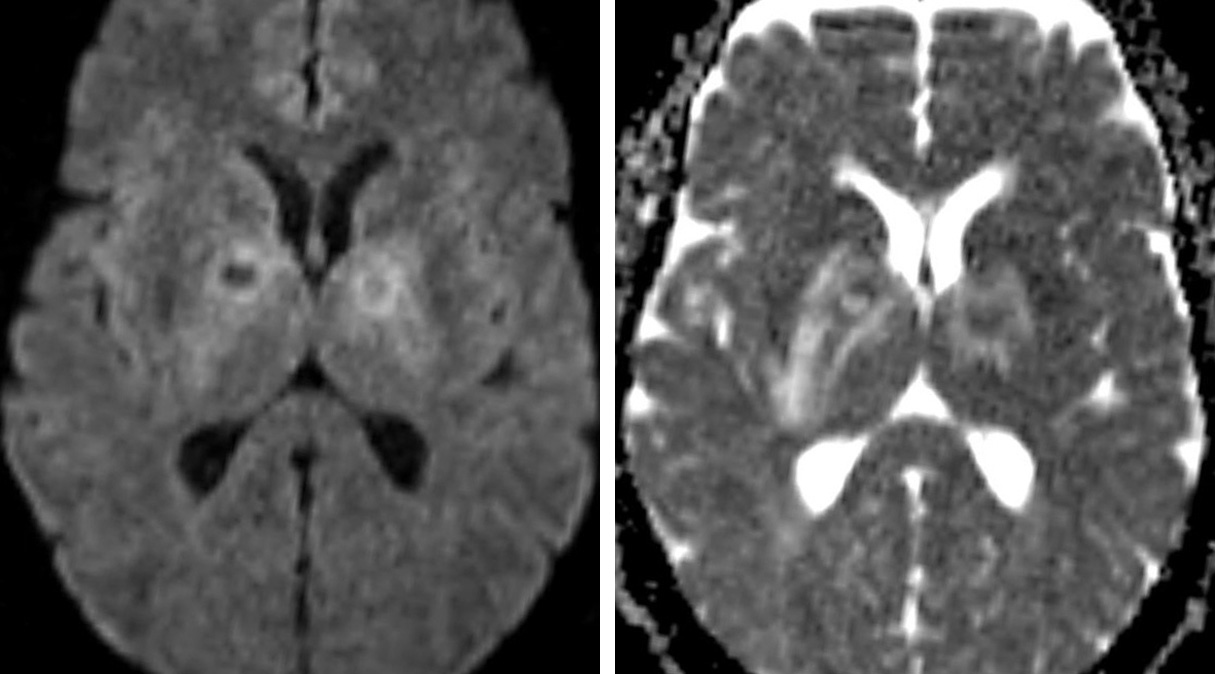
Figure 3: MR DWI/ADC: Restricted diffusion in the rim of the lesion (not centrally as almost always present in pyogenic abscess). Surrounding edema seen as bright perilesional ADC and DWI signal.

Figure 4: Both lesions demonstrate central signal loss on SWI (susceptibility-weighted images) representing hemorrhage. This feature suggests toxoplasmosis over lymphoma.

Figure 5: Multiple ring-enhancing lesions are visible on contrast-enhanced MRI, predominantly distributed in the globi pallidi and at the grey-white matter junctions. The lesion in the right globus pallidus shows target-like enhancement with eccentric central enhancing nodule that is highly suggestive of toxoplasmosis, but seen in less than half of cases.
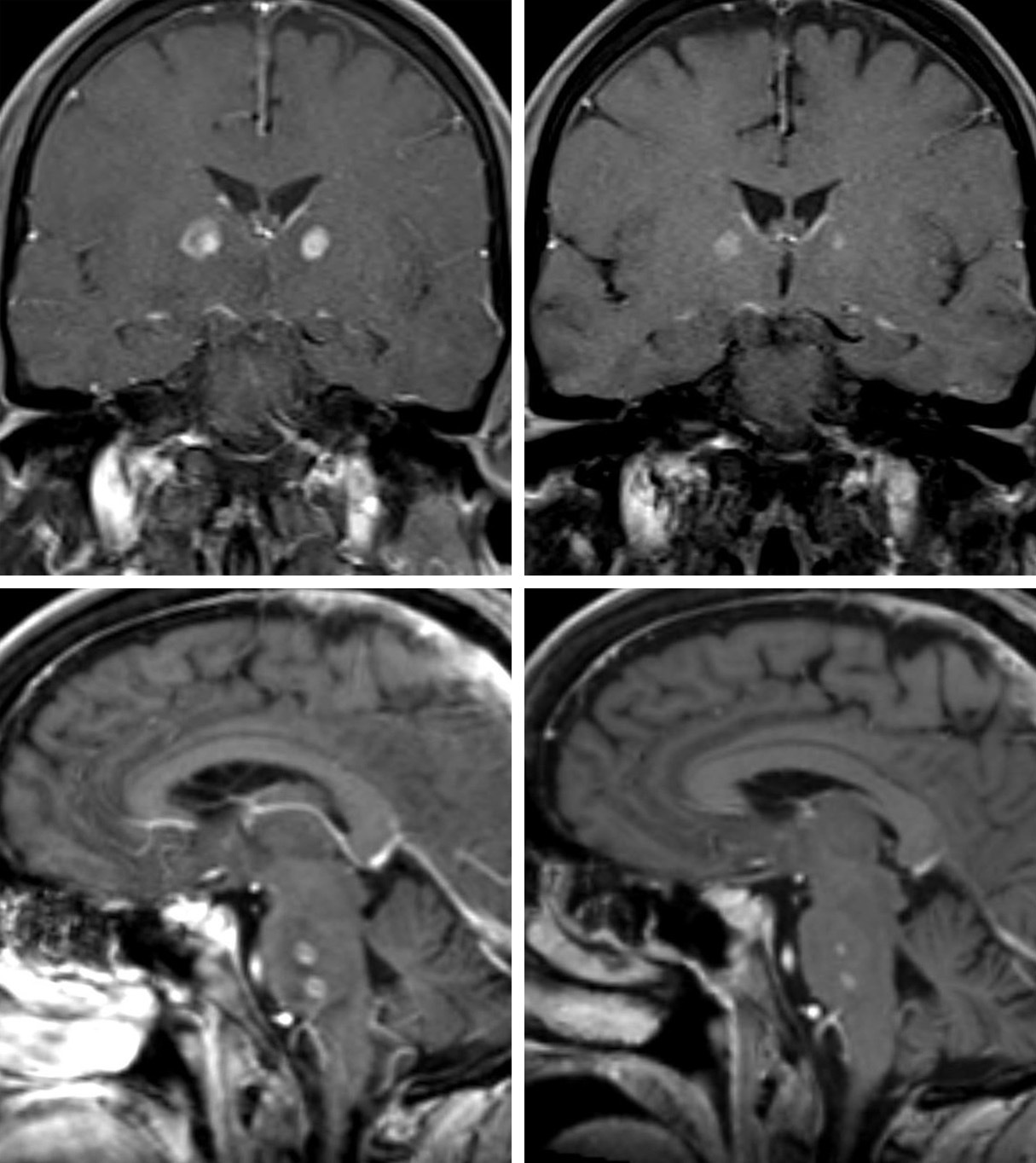
Figure 6: Coronal (top) and sagittal (bottom) T1 post-contrast imaging demonstrates enhancement in the rim of the toxoplasmosis lesions (left), improved after 2 months of antiparasitic therapy (right).
Differential Diagnosis
- Primary CNS lymphoma
- Metastases
- Other infections:
- Cryptococcosis
- Pyogenic abscesses (septic emboli)
- Tuberculosis
- Neurocysticercosis
For more information, please see the corresponding chapter in Radiopaedia. and the Toxoplasmosis chapter in the Brain Tumor Mimics sub-volume within the Neurosurgical Atlas.
Contributor: Jordan McDonald, MD
References
Chang L, Miller ML, McBride D, et al. Brain lesions in patients with AIDS: H-1 MR spectroscopy. Radiology. 1995;197(2):525-531.
Dina TS. Primary central nervous system lymphoma versus toxoplasmosis in AIDS. Radiology 1991;179(3):823-828.
Ionita C, Wasay M, Balos L, Bakshi R. MR imaging in toxoplasmosis encephalitis after bone marrow transplantation: paucity of enhancement despite fulminant disease. AJNR Am J Neuroradiology. 2004;25(2):270-273.
Kim HW, Won KS, Choi BW, Zeon SK. Cerebral Toxoplasmosis in a Patient with AIDS on F-18 FDG PET/CT. Nucl Med Mol Imaging. 2010 Apr; 44(1): 75-77. doi: 10.1007/s13139-009-0014-3
Lee GT, Antelo F, Mlikotic AA. Best cases from the AFIP: cerebral toxoplasmosis. RadioGraphics. 2009; 29 (4): 1200-1205. doi: 10.1148/rg.294085205
Lorberboym M, Wallach F, Estok L, et al. Thallium-201 retention in focal intracranial lesions for differential diagnosis of primary lymphoma and non-malignant lesions in AIDS patients. J Nucl Med 1998; 39(8):1366-1369.
Pomper, M. G., Constantinides, C. D., Barker, P. B., Bizzi, A., Dobgan, A. S., Yokoi, F., Wong, D. F. (2002). Quantitative MR spectroscopic imaging of brain lesions in patients with AIDS: Correlation with [11C-methyl]thymidine pet and thallium-201 SPECT. Academic Radiology, 9(4), 398-409.
Smith AB, Smirniotopoulos JG, Rushing EJ. From the Archives of the AFIP -- Central Nervous System Infections Associated with Human Immunodeficiency Virus Infection: Radiologic-Pathologic Correlation. RadioGraphics. 2008; 28:2033-2058. doi: 10.1148/rg.287085135
Please login to post a comment.




