

Abducens Nerve

ABSTRACT
The aim of this study is to demonstrate and review the detailed microsurgical anatomy of the abducens nerve and surrounding structures along its entire course and to provide its topographic measurements. Ten cadaveric heads were examined using ×3 to ×40 magnification after the arteries and veins were injected with colored silicone. Both sides of each cadaveric head were dissected using different skull base approaches to demonstrate the entire course of the abducens nerve from the pontomedullary sulcus to the lateral rectus muscle. The anatomy of the petroclival area and the cavernous sinus through which the abducens nerve passes are complex due to the high density of critically important neural and vascular structures. The abducens nerve has angulations and fixation points along its course that put the nerve at risk in many clinical situations. From a surgical viewpoint, the petrous tubercle of the petrous apex is an intraoperative landmark to avoid damage to the abducens nerve. The abducens nerve is quite different from the other nerves. No other cranial nerve has a long intradural path with angulations and fixations such as the abducens nerve in petroclival venous confluence. A precise knowledge of the relationship between the abducens nerve and surrounding structures has allowed neurosurgeon to approach the clivus, petroclival area, cavernous sinus, and superior orbital fissure without surgical complications.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
INTRODUCTION
Surgical interventions of skull base lesions have been increasingly performed in the last several years. The microsurgical anatomy of the abducens nerve is important for clinical reasons and surgical approaches because it is located in the petroclival area and cavernous sinus, which are the most complex regions of the skull base. From the origin to the termination of the abducens nerve, it courses along the subarachnoid space (Iaconetta et al., 2007), petroclival region (Ozveren et al., 2002a, 2003; Iaconetta et al., 2003; Ozer et al., 2010), cavernous sinus (Iaconetta et al., 2001, 2007; Jittapiromsak et al., 2010), and orbit (Iaconetta et al., 2007; Shi et al., 2007). The abducens nerve has a long intracranial course along the vascular, neural, ligamentous, and bony structures and is very vulnerable to direct and indirect injury (Takagi et al., 1976; Antoniades et al., 1993; Lazow et al., 1995; Ziyal et al., 2003). The abducens nerve usually exits the pontomedullary sulcus of the brainstem as a single trunk. However, it may split into duplicated branches along its course. The incidence of duplication has been reported in the literature to range from 5% to 28.6% (Nathan et al., 1974; Marinkovic et al., 1994). In the presence of duplication or variations of the abducens, care should be taken to prevent surgery-related risks and complications. Preoperative diagnosis of the duplicated abducens nerve is possible through thin slice magnetic resonance imaging (Alkan et al., 2004).
An exact knowledge of the anatomy of the abducens nerve and its surrounding connective and neurovascular structures would be helpful for surgeons who need to explore the petroclival region, cavernous sinus, and superior orbital fissure (SOF) using the transcranial and endoscopic approaches. The purpose of this anatomical study is to review the entire anatomy of the abducens nerve and its surrounding connective and neurovascular structures from the brainstem to the lateral rectus muscle.
MATERIALS AND METHODS
Ten adult cadaver heads (20 specimens) were used for microsurgical dissection. After fixation of the cadaver heads with formaldehyde, both common carotid arteries, vertebral arteries, and internal jugular veins were dissected and cannulated with polyethylene catheters, and debris or chemicals were thoroughly removed with saline solution. The vessels were injected with a colored silicone mixture, red for arteries and blue for veins. The silicone mixture was left to harden inside the vessels for 48 hr. Next, the calvaria of heads were removed. Brains were removed meticulously, with special attention to the cranial nerves. The abducens nerve was followed to where it pierced the dura in the petroclival region. The inner layer of the dura mater around the dural entrance porus of the abducens nerve was carefully dissected to expose the course of the nerves and the venous ostia. After removal of the dura mater, the structures inside the petroclival region were dissected layer by layer and documented with photographs. The lateral wall of the cavernous sinus was removed to expose the cranial nerves. After the SOF and annulus of Zinn were opened, the nerve was entirely exposed.
Both skull base areas along the course of the abducens nerve from the 10 heads were dissected interdurally under optical magnification with the OPMI surgical microscope (Carl Zeiss Co., Oberkochen, Germany). An EOS 50D camera (Canon, Tokyo, Japan) was used for photographic documentation.
RESULTS
The abducens nerve consists of subarachnoid, petroclival, intracavernous, and orbital portions. The interdural petroclival and intracavernous parts course between the dural layers of the skull base, and their anatomy is more complex than the other parts.
Subarachnoid Segment
The abducens nerve leaves the brainstem at the junction of the pons and the medulla, medial to the facial nerve. The nerve enters the subarachnoid space when it emerges at the pontomedullary sulcus which is located 4.35 mm (range, 3.0–5.8 mm) from the midline of the brainstem (Fig. 1C and 1D). This segment courses upward, anteriorly and laterally between the pons and clivus, and then pierces the inner layer of dura mater located inferomedial to the dural entrance porus of the trigeminal nerve to enter the interdural petroclival venous confluence (PVC; Iaconetta et al., 2003). The average length and diameter of this segment are 15.8 mm (range, 12.8–19.1 mm) and 1.31 mm (range, 0.8–1.7 mm), respectively. The external reflection of the petroclival dura mater forms both the dural entrance porus and the dural sleeve of the abducens nerve (Fig. 1E and 1F). The diameter of the dural entrance porus of the abducens nerve is 1.63 mm (range, 1.1–2.1 mm). The arachnoid membrane, which extends onto the clivus and forms the anterior wall of the prepontine cistern, is reflected anteriorly into the dural entrance porus of the abducens nerve and follows the nerve inside the dural sleeve.
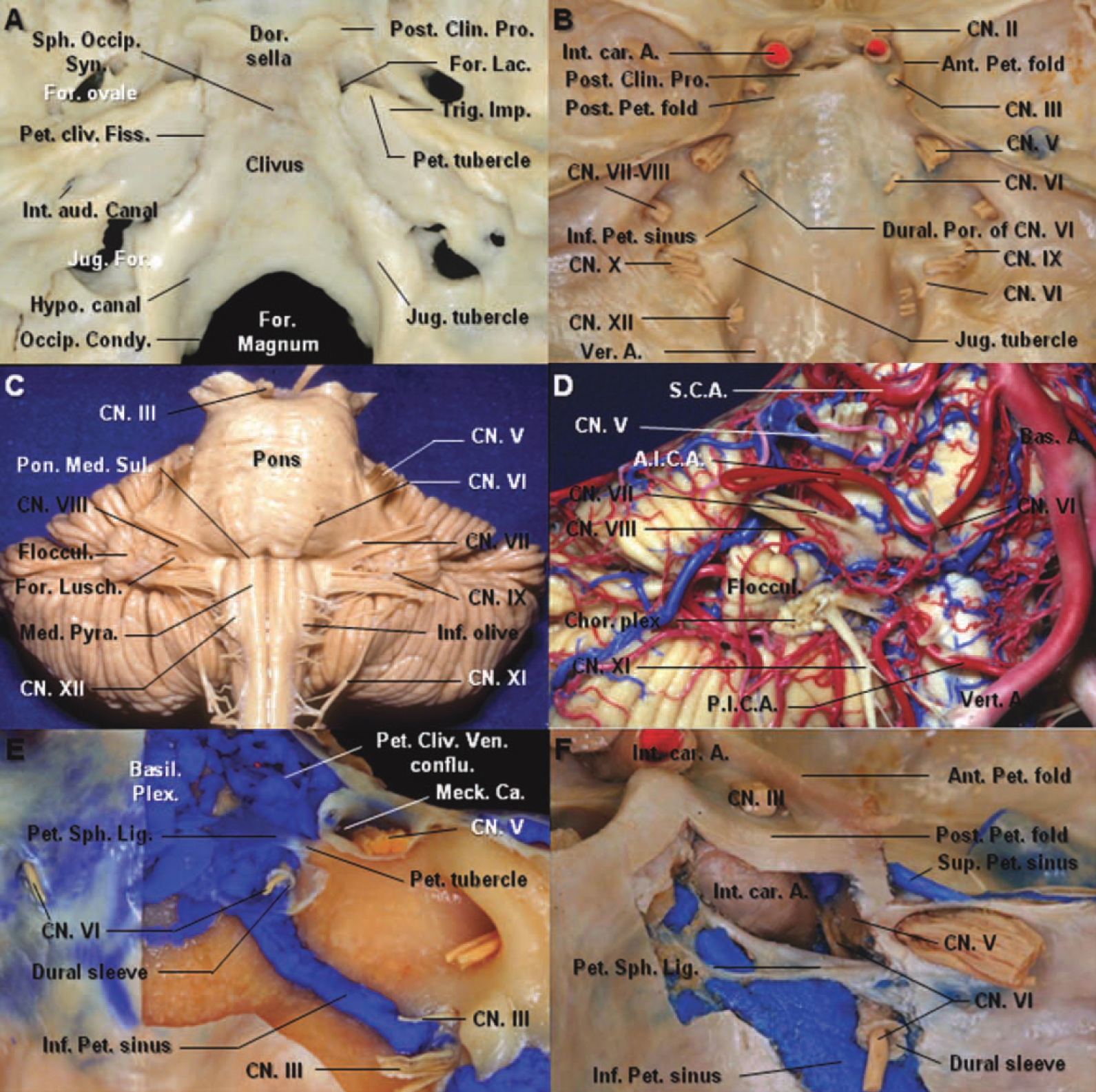
Figure 1. A: The petrosal apex of the temporal bone is received into the angular interval between the clival part of the occipital bone and the greater wing of the sphenoid bone. The apex of the petrous bone presents the internal orifice of the internal carotid artery and forms the posterolateral border of the foramen lacerum. The petrous tubercle, the insertion of the petrosphenoid ligament, is medial to the trigeminal impression. B: The brain has been removed to expose the foramina for the cranial nerves. The abducens nerve enters the dural porus of the abducens and Dorello’s canal located medial and inferior to the porus of the trigeminal nerve. The Inferior Petrosal Sinus courses medial to the abducens nerve. C: Anterior view of the brainstem. The abducens nerve leaves the brainstem at the junction of the pons and the medulla, medial to the facial nerve. It course upward, anteriorly and laterally between the pons and clivus within pontine arachnoid. D: The anterior inferior cerebellar artery passes dorsal to the abducens nerve. The vein of the pontomesencephalic sulcus courses below the abducens nerve. E: The meningeal dural layer of the posterior aspect of the petrous apex has been removed to expose the dural sleeve of the abducens nerve, petroclival venous confluence, basilar plexus, and inferior petrosal sinus. The inferior petrosal sinus connects the petroclival venous confluence with the jugular bulb and courses medial to the abducens nerve. The abducens nerve passes under the petrosphenoid ligament. F: The petroclival venous confluence has been removed. The abducens nerve enters the cavernous sinus between the internal carotid artery and the trigeminal nerve. The cisternal space follows the nerve inside the dural sleeve. The petrosphenoid ligament is attached laterally to the petrous tubercle medial to the trigeminal nerve. A., artery; Ant., anterior; Aud., auditory; Bas., basilar; Ca., cave; Chor., choroid; Clin., clinoid; CN., cranial nerve; conflu., confluence; Condy., condyle; Dor., dorsum; For., foramen; Hypo., hypoglossal; Imp., impression; Inf., inferior; Int., internal; Jug., jugular; Lac., lacerum; Lig., ligament; Meck., Meckel’s; Med., medulla; Occip., occipital; Pet., petroclinoid; Petro., petrosal; Plex., plexus; Pon., pons; Por., porus; Post., posterior; Pro., process; Pyr., pyramid; Sin., sinus; Sph., sphenoid; Sul., sulcus; Syn., synostosis; Ven., venous; Ver., vertebral. (Images courtesy of AL Rhoton, Jr.)
The anterior pontine segment of the anterior inferior cerebellar artery passes ventral to the abducens nerve in 85% of the cases, and dorsal to the nerve in 15% (Fig. 1D). In our specimens, we did not find any artery supplying the cisternal segment of the abducens nerve.
Petroclival Segment
After piercing the inner layer of the petroclival dura, the abducens nerve progressively courses in a horizontal and somewhat straight direction at the dural entrance porus to the petrous apex (1st genu) and passes through the interdural venous confluence, which is named the sphenopetroclival venous confluence (SPCVC; Destrieux et al., 1997; Iaconetta et al., 2003). The SPCVC is located at the junction of the posterior part of the cavernous sinus, the lateral part of the basilar plexus, and anterior part of the superior and inferior petrosal sinus (SPS and IPS; Figs. 1B, 1E, and 1F and 2A–2F). The majority of the basilar plexus is located between the layers of the dura mater on the clivus and extends from the dorsum sella to the midportion of the clivus. Venous space islands may present between the midportion of the clivus and the foramen magnum. It is the largest and most constant intercavernous connection across the midline and connects the posterior aspect of both cavernous sinuses. The SPS passes above the dural entrance porus of the trigeminal nerve and is located between the meningeal dura and dorsolateral wall of Meckel’s cave. It connects the SPCVC and the posterior part of the cavernous sinus with the junction of the transverse and sigmoid sinus. The IPS, which is situated in the petroclival fissure, connects the SPCVC with the jugular bulb (Fig. 1B, 1E, and 1F). In 16 of the 20 specimens (80%), the main portion of the IPS opening into the SPCVC is lateral to the dural porus of the abducens, and in the remaining four specimens (20%), it is medial to this dural porus. The dural entrance porus of the abducens nerve was surrounded with the blood of the IPS.

Figure 2. Stepwise dissections of the petrous apex area. A: Anterolateral view of the petrous apex. The dura layer forming the roof of the cavernous sinus has been removed to expose the oculomotor and trochlear nerve. B: The meningeal layer of the dura has been excised to expose the posterior clinoid process and is reflected posteromedially with the suture. C: The reflected dura layer has been removed along the clivus to open the entrance point of the abducens nerve into the dura. D: After removing the meningeal layer of the dura, blue silicone indicating the petroclival venous confluence has been exposed. E,F: The petroclival venous confluence has been removed to expose the petrosphenoid ligament. The petrosphenoid ligament attaches to the petrous tubercle laterally and to the dura sleeve for the abducens nerve inferiorly. The dorsal meningeal artery arising from the meningohypophyseal trunk passes posteriorly along the medial aspect of the abducens nerve. A., artery; Cav., cavernous; Car., carotid; Clin., clinoid; Cliv., clival; CN., cranial nerve; Conflu., confluence; Dor., dorsal; Gang., ganglion; Lig., ligament; Mening., meningeal; MHT., meningohypophyseal trunk; Petro., petrosal; Post., posterior; Pro., process; Seg., segment; Sin., sinus; Sph., sphenoid; Tri., triangle; Ven., venous. (Images courtesy of AL Rhoton, Jr.)
The anterior margin of the SPCVC is a coronal plane passing through the posterior petroclinoid fold superiorly and the posterior wall of the vertical segment of the cavernous carotid artery inferiorly. The posterior margin is the meningeal layer of the petroclival dura. The medial margin is a sagittal plane passing through the lateral edge of the dorsum sella anteriorly to the dural entrance porus of the abducens nerve posteriorly and inferiorly. The lateral limit of the SPCVC is the medial edge of Meckel’s cave. The inferior limit is the line passing through the dural entrance porus of the abducens and trigeminal nerves. The mean distance between the entry points of the trigeminal and abducens nerves is 9.41 mm (range, 6.4–12.5 mm; Figs. 2 and 3C and 3D).

Figure 3. A: Lateral view. The lateral wall of the cavernous sinus extends downward from the tentorial edge and blends into the dura covering Meckel’s cave and the middle fossa. The outer layer of dura has been peeled away from the lateral wall of the cavernous sinus and Meckel’s cave. This exposes the trigeminal nerve. B: The thin layer covering Meckel’s cave consists in part of the arachnoid membrane extending forward from the posterior fossa and surrounding trigeminal nerve to the level of the trigeminal ganglion. C: Superior view. The subarachnoid segment of the abducens nerve courses upward, anteriorly and laterally between the pons and clivus, and then pierces the inner layer of the dura mater located inferomedial to the dural entrance porus of the trigeminal nerve to enter the interdural petroclival venous confluence. The SPS passes above the ostium of Meckel’s cave and joins the posterior part of the cavernous sinus. D: Exiting Dorello’s canal, the abducens nerve enters the cavernous sinus. The abducens nerve is attached to the posterior vertical segment of the cavernous carotid artery by connective tissue. The trigeminal nerve has been retracted laterally to expose the petrolingual ligament, spanning from the lingula of the sphenoid bone anteriorly to the petrous apex posteriorly and covering the superiolateral surface of the lacerum segment of the carotid artery. The basilar plexus is located between the layers of the dura mater on the clivus and extends from the dorsum sella to the anterior rim of the foramen magnum. A., artery; ACP., anterior clinoid process; Ant., anterior; Bas., basilar; Car., carotid; Cav., cavernous; CN., cranial nerve; Conflu., confluence; For., foramen; GSPN., great superficial petrosal nerve; Hypo., hypophyseal; Inf., inferior; Lat., lateral; Lig., ligament; Ling., lingual; MMA., middle meningeal artery; Pcom., posterior communicating; PCP., posterior clinoid process; Pet., petroclinoid; Pitu., pituitary; Plex., plexus; Post., posterior; Rotund., rotundum; SPS., superior petrosal sinus; Sph., sphenoid; Tr., trunk; Ven., venous. (Images courtesy of AL Rhoton, Jr.)
The SPCVC contains the petrosphenoid ligament (Gruber’s ligament), the petroclival segment and dural sleeve of the abducens nerve, and the dorsal meningeal artery (Fig. 2C–2F). The petrosphenoid ligament travels parallel to the petroclival dura mater and is attached to the posterior clinoid process and superolateral part of the clivus anteromedially and to the petrous tubercle, the medial border of the trigeminal impression in the petrous apex, posterolaterally (Iaconetta et al., 2001). The mean distance between the abducens nerve and petrous tubercle is 2.80 mm (range, 1.4–9.5 mm; Fig. 2).
The petrosphenoid ligament has a butterfly shape, with its midpoint being narrow and consisting of dense collagen fibers (Fig. 2E and 2F). The widths of the medial and lateral insertion of the ligament were 3.85 mm (range, 1.8–6.4 mm) and 3.0 mm (range, 1.7–5.7 mm), respectively. At the midpoint of the ligament, the width was found to be 2.05 mm (range, 1.1–3.3 mm). Its length was measured at 11.05 mm (range, 7.5–14.5 mm). A narrow space was filled with the blood between the petrosphenoid ligament and the meningeal layer of the petroclival dura mater. This ligament divided the SPCVC into two spaces: superior (between the ligament and posterior petroclinoid fold) and inferior (between the ligament and the bone groove; Fig. 2). In 5 of 20 specimens (25%), it was found to be ossified (Fig. 3). The dural sleeve of the abducens nerve, the dorsal meningeal artery or its branches, and the venous blood space were located under the petrosphenoid ligament in our study (Fig. 2C–2F).
In 95% of 20 specimens, the dural sleeve of the abducens nerve courses the lateral half of Dorello’s canal, limited by the lateral edge of the dorsum sella medially, the petrosphenoid ligament superiorly, the superior aspect of the upper clivus inferiorly, and the petrous apex laterally. The dural sleeve passes the medial half in 5% of the specimens. The dural sleeve was thick around the dural entrance porus and thinner at the apex of Dorello’s canal. It covers the abducens nerve between the dural entrance porus and the anterior margin of the petrosphenoid ligament. Its length was 9.18 mm (range, 6.8–12.4 mm). The dural sleeve was attached to the inferior aspect of the petrosphenoid ligament and extended into the cavernous sinus as a fibrous layer covering the nerve up to the lateral rectus muscle (Fig. 2E and 2F). At the petrous apex, the nerve courses inferiorly and laterally to form the 2nd genu and reaches the lateral aspect of the vertical segment of the intracavernous carotid artery. The length of the petroclival segment of the abducens is 11.34 mm (range, 8.9–13.4 mm; Fig. 4).

Figure 4. Lateral view of the petrous apex. A: The arachnoid covering of Meckel’s cave, which extends forward around the posterior trigeminal root to the level of the midportion of the ganglion. The superior petrosal sinus above the posterior trigeminal root has been removed. The abducens nerve passes under the lateral part of the ossified petrosphenoid ligament to enter the cavernous sinus. B: The ophthalmic nerve has been retracted laterally. The abducens nerve continues running medial to the ophthalmic nerve in the cavernous sinus and runs superiorly and parallel to the petrolingual ligament before it exits through the superior orbital fissure. The inferolateral trunk arises from the lateral side of the midportion of the horizontal segment of the intracavernous carotid. It passes lateral to the abducens nerve and medial to the first trigeminal division. After the internal carotid artery passes through the petrolingual ligament, the sympathetic plexus is observed in the anterolateral aspect of the proximal vertical segment of the cavernous carotid artery. The plexus anastomose with the cavernous segment of the abducens nerve. C: Anterior view of a coronal section in front of the sphenoid sinus, through the orbits and pterygoid processes. The pituitary gland, intracavernous carotids, optic nerve, and cavernous sinus have been exposed by removing the bone of the sinus wall. The upper part of the clivus has been removed to expose the basilar plexus. The periarterial sympathetic plexus courses upward along the posterior vertical segment of the cavernous carotid artery. D: Anterior oblique view of the coronal section. The petroclival venous confluence has been removed to expose the abducens nerve. After entering the dura, the abducens nerve courses in a somewhat straight direction to reach the petrous apex. The abducens nerve has a pseudobranching pattern which has no intervening tissue in the cavernous sinus and anastomoses with the periarterial sympathetic plexus. A., artery; Bas., basilar; Car., carotid; CN., cranial nerve; For., foramen; Gl., gland; GSPN., great superficial petrosal nerve; Hypo., hypophyseal; Inf., inferior; Lat., lateral; Lig., ligament; N., nerve; Oph., ophthalmic; Opt., optic; PCP., posterior clinoid process; Pitu., pituitary; Plex., plexus; Sin., sinus; Sph., sphenoid; SOF., superior orbital fissure; Str., strut; Sympath., sympathetic; Tent., tentorial; Tr., trunk. (Images courtesy of AL Rhoton, Jr.)
The dorsal meningeal artery and its branches arising from the meningohypophyseal trunk at the posterior genu of the intracavernous carotid artery courses medial to the abducens nerve, passing under the petrosphenoid ligament in 75% of the cases. Although it has been known that the dorsal meningeal artery provides the blood supply to this segment of the abducens nerve, we did not find any direct communication between the nerve and artery in the interdural petroclival area (Dolenc, 1987).
Cavernous Segment
Exiting Dorello’s canal, the abducens nerve enters the cavernous sinus. The external layer (periosteal layer) of the lateral wall of the cavernous sinus is thicker with a pearly gray color, whereas the internal layer (cerebral layer) is thin, transparent, and contains the oculomotor, trochlear, and trigeminal nerves on their way through the cavernous sinus and the SOF (Fig. 3). The nerve bends laterally around the proximal portion of the intracavernous carotid artery (3rd genu) and gently ascends as it passes forward inside the cavernous sinus medial to the ophthalmic nerve, on the lateral side of the internal carotid artery. The nerve contacts the lateral wall of the cavernous segment of the ICA medially and the medial wall of Meckel’s cave laterally. The abducens nerve has the most medial site of entry of the nerves coursing in the cavernous sinus wall and maintains that position in its course through the sinus (Figs. 3C and 4). The abducens nerve continues running medial and inferior to the ophthalmic nerve in the cavernous sinus and runs superiorly and parallel to the petrolingual ligament before it exits through the SOF (Fig. 4A and 4B).
The periarterial sympathetic plexus, a network of neural fibers, adheres to the petrous segment of the ICA with a very thin layer of periarterial connective tissue. Shortly after the ICA passes through the petrolingual ligament, the sympathetic plexus is observed in the anterolateral aspect of the proximal vertical segment of the cavernous carotid artery. Following the end of the dural sleeve, the abducens nerve anastomoses with the branches of the sympathetic plexus on the lateral wall of the cavernous segment of the ICA and with the trigeminal nerve to form the 3rd genu (Fig. 4). The plexus then runs together with the ophthalmic nerve to reach the pupilodilator through long ciliary nerves, the branches of the nasocillary nerve (Ozveren et al., 2001). The abducens nerve is attached to the posterior vertical segment and the beginning of the anterior bend of the cavernous carotid artery by connective tissue. In that area, the round shape of the proximal abducens nerve changes to a flat vertical configuration, and the nerve may be split into multiple bundles. In our specimens, the cavernous segment of the abducens nerve split into two bundles in 25% of the cases and into three bundles in 10%. Before exiting the cavernous sinus, the duplicated nerves fused into a single trunk at the level of the horizontal portion of the ICA (Fig. 4B–4D).
The inferolateral trunk (the artery of the inferior cavernous sinus) arises from the lateral side of the midportion of the horizontal segment of the intracavernous carotid 6.30 mm (range, 3.8–8.5 mm) distal to the origin of the meningohypophyseal trunk. It passes lateral (90%) or medial (10%) of the abducens nerve, provides branches to the abducens nerve, and courses downward medial to the first trigeminal division to supply the dura of the inferior lateral wall of the cavernous sinus. The mean distance between the abducens nerve and the origin of the inferolateral trunk is 2.65 mm (range, 1.3–4.1 mm; Fig. 4). The meningohypophyseal trunk is 7.1 mm (range, 3.9–12.8 mm) from the abducens nerve and 7.58 mm (range, 5.4–12.0 mm) from Dorello’s canal. The ventral branch of the inferolateral trunk runs toward the SOF and supplies the anterior part of the cavernous segment of the abducens nerve in the vicinity of the SOF. The mean length of the cavernous segment of the abducens nerve is 27.23 mm (range, 23.1–30.2 mm).
Intraorbital Segment
This segment begins the portion of the nerve that passes through the SOF and the annulus of Zinn and ends at the insertion of the nerve into the lateral rectus muscle (Figs. 5 and 6). The abducens nerve enters the orbit via the SOF. The SOF is a small but topographically important area, which connects the middle cranial fossa and the orbit. It divides into superolateral and inferomedial parts. The abducens nerve passes through the inferomedial part of the SOF with the oculomotor nerve and nasociliary nerve (Fig. 5A–5D). The abducens travels forward in the cavernous sinus on the medial side of the ophthalmic nerve and shifts laterally below the nasociliary nerve as it passes through the inferomedial part of the SOF and annular tendon to enter the medial surface of the lateral rectus muscle. The abducens nerve is inferolateral to the nasociliary nerve, inferior to the superior division of the oculomotor nerve, and superolateral to the inferior division at the SOF. There was a fibrous septum separating the abducens nerve and the superior division of the oculomotor nerve, motor component from the nasociliary nerve, sensory component (Fig. 5D).

Figure 5. A: Superior view. The orbital roof, the periorbita and fat have been removed to expose the trochlear, frontal, and lacrimal nerves coursing in the orbital fat just beneath the periorbita. The optic canal has been unroofed and the right anterior clinoid process removed. The dura mater lines the base of the middle cranial fossa, and the cavernous sinus continues as the periorbita via the superior orbital fissure. The periorbita that covers the bones of the orbital apex, the dura lining the superior orbital fissure and the optic canal, and the fibrous components of the optic nerve sheath fuse to form the annulus of Zinn, the common tendinous ring from which the rectus muscles arise. The left dura layer that lines the lower margin of the anterior clinoid process has been excised and is reflected laterally to expose the trochlear and frontal nerves. B: Lateral view of the left superior orbital fissure. The lateral margin of the superior orbital fissure has been preserved. The abducens nerve travels through the cavernous sinus medial to the ophthalmic nerve. The abducens nerve passes through the central region of the superior orbital fissure inferomedial to the nasociliary nerve. C: Lateral view of the left orbital apex. The frontal, lacrimal, and trochlear nerves pass outside the annulus of Zinn, and the nasociliary, oculomotor, and abducens nerves pass through the tendon. D: An incision has been made in the annulus of Zinn along the medial aspect of the nasociliary nerve, which lies outside the annulus. The oculomotor nerve and its divisions are located deep and medial to the abducens nerve. The fibrous septum separates the abducens nerve from the nasociliary nerve in the annulus of Zinn. The nasociliary nerve gives rise to short ciliary nerves to the ciliary ganglion located inferolateral to the optic nerve. E: Superior view of the right orbit. The levator and superior rectus muscles have been retracted medially to expose the nasociliary and the abducens nerve. From the superior orbital fissure, the abducens nerve enters the medial surface of the lateral rectus muscle. F: The optic nerve has been retracted medially to expose the inferior division of the oculomotor nerve and the ciliary ganglion. The ciliary ganglion is situated on the inferolateral aspect of the optic nerve and on the medial side of the lateral rectus muscle. It receives three branches: the motor root from the inferior division of the oculomotor nerve, the sensory root from the nasociliary nerve, and sympathetic fibers from the plexus around the ophthalmic artery. G: The abducens nerve is divided into several branches to innervate the muscle on the medial aspect of the lateral rectus. ACP., anterior clinoid process; Cili., ciliary; CN., cranial nerve; Div., division; Fib., fibrous; Gang., ganglion; Inf., inferior; Lac., lacrimal; Lat., lateral; Lev., levator; M., muscle; N., nerve; Nasocili., nasociliary; Obl., oblique; Oph., ophthalmic; Opt., optic; Post., posterior; Rec., rectus; Str., strut; Sup., superior; V., vein. (Images courtesy of AL Rhoton, Jr.)

Figure 6. A,B,C: Coronal section parallel to the clivus through the orbital apex. The wall of the sphenoid sinus and the clivus has been removed to expose the intracavernous carotid artery and the abducens nerve. The abducens nerve runs upward, anteriorly, and laterally in the subarachnoid space, then passes through the petroclival dura and enters the petroclival venous confluence. The petroclival segment of the abducens nerve progressively courses in horizontal and straight direction. The first angulation of the abducens nerve is at the level of the dural entrance porus. The second angulation is over the petrous apex. The third angulation is at the lateral wall of the posterior vertical segment of the carotid artery. The abducens nerve shifts laterally below the nasociliary nerve as it passes through the superior orbital fissure and annular tendon to enter the medial surface of the lateral rectus muscle. D: Inferior view of the right orbit. The inferior rectus muscle has been retracted medially to expose the optic nerve, the ciliary ganglion, and the central retinal artery. The abducens nerve runs medial to the surface of the lateral rectus muscle. E: The intraorbital portion of the optic nerve has been removed. The inferior division of the oculomotor nerve is divided into three branches, innervating the medial rectus, inferior rectus, and inferior oblique muscles. F: Anterior view of the right orbit. The intraorbital portion of the optic nerve and the globe has been removed. The abducens nerve passes through the annulus of Zinn and then enters the medial surface of the lateral rectus. The nasociliary nerve crosses medially between the two divisions of the oculomotor nerve and above the optic nerve to reach the medial part of the orbit. A. artery; Bas., basilar; Car., carotid; Cen., central; Cili., ciliary; CN., cranial nerve; Div., division; Eust., Eustachian; Gang., ganglion; Gl., gland; Hypo., hypophyseal; Inf., inferior; Int., internal; Lac., lacrimal; M., muscle; Med., medial; N., nerve; Nasocili., nasociliary; Obl., oblique; OCR., opticocarotid recess; Pitu., pituitary; Oph., ophthalmic; Rec., rectus; Ret., retinal; Sup., superior; Sympath., sympathetic. (Images courtesy of AL Rhoton, Jr.)
At the level of the SOF, the nasociliary nerve arising from the medial side of the ophthalmic nerve gently ascends laterally to the inferior division of the oculomotor nerve and then crosses medially between the two divisions of the oculomotor nerve and above the optic nerve to reach the medial part of the orbit. At the apex of the orbit, the nasociliary nerve and the inferior division of the oculomotor nerve curve medially as the abducens nerve shifts laterally to reach the medial surface of the lateral rectus muscle (Figs. 5 and 6). The abducens nerve was divided into three to five branches to innervate the muscle on the medial aspect of the lateral rectus muscle. The branches of the abducens nerve ended on the posterior one-third of the lateral rectus in 80% of the specimens and on the middle one-third in the remaining 20%. The length of the orbital segment of the abducens nerve is 13.35 mm (range, 10.2–17.5 mm; Figs. 5 and 6).
DISCUSSION
The abducens nerve (VI) has a long intracranial course and can therefore be affected by many pathological lesions, including conditions that cause changes of intracranial pressure (Takagi et al., 1976; Black and Chapman, 1981; Umansky et al., 1992; Berlit et al., 1994; Krisht et al., 1994; Ziyal et al., 2003; Ayberk et al., 2008). However, the trochlear nerve, which also has a much longer path after it originates posteriorly from the tectum of the midbrain, is rarely injured in patients with hydrocephalus. This is why other mechanisms, rather than the length of the cranial nerve are involved in the development of abducens nerve palsy (Hanson et al., 2004). The aim of this study is to investigate the path and the surrounding anatomic relationship of the entire abducens nerve along its course.
Umansky et al. (1991, 1992) suggested the long intracranial course of the abducens nerve, its tortuosity, and its tight attachment to the skull base at the level of the petrous apex explained the vulnerability of the nerve to some pathological conditions. Recent anatomic report showed membranous coverage surrounding petroclival segment of the abducens nerve rigidly fixated the nerve as it traversed Dorello canal, thereby not allowing any movement (Tubbs et al., 2011). We observed three angulations of the nerve along its course from the external brainstem to the cavernous sinus and several attachments of the nerve to the surrounding structures. The first angulation is at the level of the dural entrance porus.
The nerve runs upward, anteriorly, and laterally in the subarachnoid space, then passes through the dura mater and enters the SPCVC. Its direction changes in the confluence, and it progressively courses in a horizontal and straight direction. The second angulation is over the petrous apex, where the nerve courses downward and laterally to reach the lateral wall of the posterior vertical segment of the cavernous carotid artery. The third angulation is at the lateral wall of the posterior vertical segment of the carotid artery, where the abducens nerve has connection with the periarterial sympathetic plexus. Umansky et al. (1992) observed the most severe angulation and main fixation point at the petrous apex, the second angulation. The fixation of the petroclival and cavernous parts of the abducens nerve were thought to be tethering points, resulting in nerve palsy in patients with an intracranial tumor as a false localizing sign (Ro et al., 1995; Ayberk et al., 2008; Tubbs et al., 2011). Pathological conditions shifting the brainstem, such as spontaneous intracranial hypotension or hypotension secondary to the shunting procedure to treat hydrocephalus, were reported to lead to the development of abducens nerve palsy by stretch force (Black and Chapman, 1981; Ayberk et al., 2008). The mechanism of these nerve palsies is thought to be compression of the abducens nerve against the dural entrance porus and petrous apex by retraction related to the downward migration of the brainstem (Rush and Younge, 1981; Miller et al., 1982).
Abducens nerve palsy may develop during endovascular surgery via the transvenous route of the IPS (Oishi et al., 1999). In cases of the abducens nerve occupying the medial half of Dorello’s canal, the nerve is in the path of the catheter, which may result in damage to the nerve (Ozveren et al., 2002a). We found the presence of the abducens nerve in the medial half of Dorello’s canal in only 5% of the 20 specimens. Additionally, the relatively low incidence of isolated abducens nerve palsy after the use of a transvenous route through the IPS may be related to the protection of the abducens nerve by its dural sleeve. The thickness of the dural sleeve of the abducens nerve may be important in nerve damage caused by a catheter (Ozveren et al., 2002a). The membranous protection of the abducens nerve in the petroclival region makes the nerve resistant to pathology. However, this membranous coverage attenuates inside the cavernous sinus beyond the petrous apex. Therefore, the abducens nerve seems to resist the invasion of petroclival masses compared with intracavernous lesion because of its membranous coverage (Ozveren et al., 2002b).
Despite continuous improvements in neurosurgical knowledge, the definitions of the boundaries of Dorello’s canal are being debated. Dorello’s canal was first described by Gruber (1859) as an osteofibrous canal at the apex of the petrous bone containing the abducens nerve and the IPS. In 1905, Dorello described the canal as the anatomic region between the petrous apex and the petrosphenoid ligament (Dorello, 1954). Nathan et al. (1974) defined the canal as the small space limited by the petrous apex, the petroclinoid ligament, and the dorsum sella. Early studies described Dorello’s canal as a short, osteofibrous channel between the petrous apex and Gruber’s (petrosphenoid) ligament (Dorello, 1954; Piffer and Zorzetto, 1980; Tsitsopoulos et al., 1996; Lang, 2001). Although it has been reported that the abducens nerve passes under the petrosphenoid ligament, some studies showed that the branches of the abducens nerve coursed above it (Jain, 1964; Nathan et al., 1974). Later, investigators defined Dorello’s canal as a larger anatomic space of the petrous apex between the inner and outer layer of the petroclival dura mater (Umansky et al., 1991; Fukushima et al., 1996; Destrieux et al., 1997; Ono et al., 2004). Destrieux et al. proposed to name the area, located between the cerebral and periosteal layers of the petroclival dura mate, the PVC instead of the Dorello’s canal. The abducens nerve courses from the dural entrance porus to the posterior part of the cavernous sinus through the PVC (Destrieux et al., 1997). Classically, Dorello’s canal is defined as being located inside a PVC formed by the junction of the posterior cavernous sinus, basilar sinus, and the IPS. Therefore, the petrosphenoid ligament is immersed in the venous confluence (Iaconetta et al., 2003).
The petrosphenoid ligament (Gruber’s ligament) is an important structure in the petroclival area, not only from an anatomical point of view but also in surgical and endovascular practice. This ligament fixes the sheath of the abducens nerve in the PVC. The abducens nerve is protected by the petrosphenoid ligament during the drilling of the petrous bone (Ozveren et al., 2002a). The ligament travels parallel to the petroclival dura mater, attaches inferior to the posterior clinoid process at the level of the lateral aspect of the dorsum sella, and runs toward the apex of the petrous apex. The petrolingual ligament spans from the lingula of the sphenoid bone anteriorly to the petrous apex posteriorly and covers the superolateral surface of the lacerum segment of the ICA. The complex of the superior sphenopetrosal (Gruber’s) ligament and inferior sphenopetrosal (petrolingual) ligament constitute a falciform ligament (Iaconetta et al., 2003, 2007).
The variations of the abducens nerve may have some practical surgery-related implications. The abducens nerve usually leaves the brainstem as a single trunk. However, the incidence of a duplicated abducens nerve has been reported to range from 8% to 18% (Jain, 1964; Nathan et al., 1974; Iaconetta et al., 2001). Nathan et al. proposed three course patterns of the abducens nerve. In Type I (86.5%), the nerve emerges from the brainstem as a single trunk that reaches the lateral rectus. Type II abducens nerve (6%) leaves the brainstem as a single trunk and splits into two branches in its cisternal segment. They pierce the dura mater separately, merge to form a single trunk, and enter the orbit. In Type III (7.5%), the nerve originates as two separate trunks fusing again into the cavernous sinus (Nathan et al., 1974). Jain (1964) identified another anatomical variation in which the abducens nerve emerges from the brainstem as two branches that travel anteriorly, and innervate the lateral rectus muscle separately. In this study, we found the incidence of a duplicated abducens nerve to be 35% in the cavernous segment. Based on the classification proposed by Nathan et al., our all specimens belonged to the Type I. In Types II and III, the abducens branches pierce the dura through separate entrance porus and travel independently with intervening tissue and then reunite. The branching anatomy of the abducens nerve at the cavernous portion which has no intervening tissue is labeled ‘‘pseudobranching.’’ Pseudobranching is perhaps caused by pressure of the ICA against the nerve at its angulation at the carotid angle (Ozer et al., 2010). True branching and duplication are probably congenital (Iaconetta et al., 2001).
The blood supply of the abducens nerve has been well known (Dolenc, 1987; Krisht et al., 1994; Marinkovic et al., 1994). Marinkovic et al. reported that the blood supply of the subarachnoid segment was contributed by the anterolateral arteries (85.71%), especially by those arising from the perforating branches of the basilar artery. The anterior inferior cerebellar artery supplied 14.29% of the subarachnoid segment, and the pontomedullary artery supplied only 7.14% of them (Marinkovic et al., 1994). The petroclival portion is supplied by the dorsal meningeal branch of the meningohypophyseal trunk. The cavernous and orbital portions receive their blood supply from the ophthalmic branch of the inferolateral trunk, the artery of the inferior cavernous sinus. However, in this study, no branch of the dorsal meningeal artery penetrated the abducens nerve through the dural and arachnoid coverages at the petroclival confluence. Yasargil (2002) described that cranial nerves with their arteries and veins advance in the form of arachnoid packs in their own foramina. The extension of the subarachnoid space into Dorello’s canal indicates that the abducens nerve is supplied through the tiny arterioles at the subarachnoid space, through the CSF, or both (Ozveren et al., 2002b, 2007).
From a surgical point of view, the abducens nerve is located just below and medial to the petrous tubercle, the anterior border of the trigeminal impression of the petrous apex. The petrous tubercle is an optimal intraoperative landmark to use for avoiding damage to the abducens nerve while performing a subtemporal–transtentorial–transpetrosal approach for the excision of posterior and middle fossa lesions (Icke et al., 2010). We should remember that at the level of the medial lip of Meckel’s cave, the petrous tubercle is covered by the lateral insertion of the petrosphenoid ligament, and just behind it is the abducens nerve. The early intraoperative identification of the petrous tubercle and abducens nerve could reduce surgery-related risks and complications.
CONCLUSIONS
The abducens nerve is different from other cranial nerves, especially regarding the fixation of the nerve inside the PVC and the cavernous sinus and the angulations along its entire course that put the nerve at risk for paresis in many indirect situations. The sixth nerve has a prolonged intracranial course and a close spatial relationship with the ICA. Surgeons must have detailed knowledge of the microsurgical anatomy of the petroclival area and the cavernous sinus to avoid injuring the abducens nerve and the ICA and additionally should be aware of the possibility of anatomical variations of the abducens nerve along its course to prevent nerve dysfunction.
Contributors: Wonil Joo, Fumitaka Yoshioka, Takeshi Funaki, and Albert L. Rhoton, Jr.
Content from Joo W, Yoshioka F, Funaki T, Rhoton AL, Jr. Microsurgical anatomy of the abducens nerve. Clin Anat 2012:25;1030–1042. doi.org/10.1002/ca.22047.
The Neurosurgical Atlas is honored to maintain the legacy of Albert L. Rhoton, Jr, MD.
References
- Alkan A, Sigirci A, Ozveren MF, Kutlu R, Altinok T, Onal C, Sarac K. 2004. The cisternal segment of the abducens nerve in man: Three-dimensional MR imaging. Eur J Radiol 51:218–222.
- Antoniades K, Karakasis D, Taskos N. 1993. Abducent nerve palsy following transverse fracture of the middle cranial fossa. J Craniomaxillofac Surg 21:172–175.
- Ayberk G, Ozveren MF, Yildirim T, Ercan K, Cay EK, Kocak A. 2008. Review of a series with abducens nerve palsy. Turk Neurosurg 18:366–373.
- Berlit P, Berg-Dammer E, Kuehne D. 1994. Abducens nerve palsy in spontaneous intracranial hypotension. Neurology 44:1552.
- Black PM, Chapman PH. 1981. Transient abducens paresis after shunting for hydrocephalus. Report of two cases. J Neurosurg 55:467–469.
- Destrieux C, Velut S, Kakou MK, Lefrancq T, Arbeille B, Santini JJ. 1997. A new concept in Dorello’s canal microanatomy: The petroclival venous confluence. J Neurosurg 87:67–72.
- Dolenc VV. (ed.) 1987. The blood supply of the cranial nerves in the lateral wall of the cavernous sinus. In: The Cavernous Sinus: A Multidisciplinary Approach to Vascular and Tumorous Lesions. Wien; New York: Springer-Verlag. p 67–80.
- Dorello P. 1905. Considerations about the cause of temporary abducens paralysis in inflammation of the middle ear. Atti della Clinica Oto-Rino-Laringoiatrica. Rome: Tipografia del Campidoglio. p 209–217 [in Italian].
- Fukushima T, Day JD, Hirahara K. 1996. Extradural total petrous apex resection with trigeminal translocation for improved exposure of the posterior cavernous sinus and petroclival region. Skull Base Surg 6:95–103.
- Gruber W. 1859. Contributions to the anatomy of the sphenoid and temporal bones. Schmidt’s Jahrbucher der In-Und Auslandischen: Gesammten Medicin: II. Anatomie und Physiologie. Leipzig: Verlag von Otto Wigand. p 40 [in German].
- Hanson RA, Ghosh S, Gonzalez-Gomez I, Levy ML, Gilles FH. 2004. Abducens length and vulnerability? Neurology 62:33–36.
- Iaconetta G, Fusco M, Cavallo LM, Cappabianca P, Samii M, Tschabitscher M. 2007. The abducens nerve: Microanatomic and endoscopic study. Neurosurgery 61:7–14.
- Iaconetta G, Fusco M, Samii M. 2003. The sphenopetroclival venous gulf: A microanatomical study. J Neurosurg 99:366–375.
- Iaconetta G, Tessitore E, Samii M. 2001. Duplicated abducent nerve and its course: Microanatomical study and surgery-related considerations. J Neurosurg 95:853–858.
- Icke C, Ozer E, Arda N. 2010. Microanatomical characteristics of the petrosphenoidal ligament of Gruber. Turk Neurosurg 20:323– 327.
- Jain KK. 1964. Aberrant roots of the abducent nerve. J Neurosurgery 21:349–351.
- Jittapiromsak P, Sabuncuoglu H, Deshmukh P, McDougall CG, Spetzler RF, Preul MC. 2010. Anatomical relationships of intracavernous internal carotid artery to intracavernous neural structures. Skull Base 20:327–336.
- Krisht A, Barnett DW, Barrow DL, Bonner G. 1994. The blood supply of the intracavernous cranial nerves: An anatomic study. Neurosurgery 34:275–279.
- Lang J. 1995. Skull Base and Related Structures: Atlas of Clinical Anatomy. 2nd Ed. Stuttgart: Schattauer. p 196.
- Lazow SK, Izzo SR, Feinberg ME, Berger JR. 1995. Bilateral abducens nerve palsy secondary to maxillofacial trauma: Report of case with proposed mechanism of injury. J Oral Maxillofac Surg 53:1197–1199.
- Marinkovic SV, Gibo H, Stimec B. 1994. The neurovascular relationships and the blood supply of the abducent nerve: Surgical anatomy of its cisternal segment. Neurosurgery 34:1017–1026.
- Miller EA, Savino PJ, Schatz NJ. 1982. Bilateral sixth-nerve palsy. A rare complication of water-soluble contrast myelography. Arch Ophthalmol 100:603–604.
- Nathan H, Ouaknine G, Kosary IZ. 1974. The abducens nerve. Anatomical variations in its course. J Neurosurg 41:561–566.
- Oishi H, Arai H, Sato K, Iizuka Y. 1999. Complications associated with transvenous embolisation of cavernous dural arteriovenous fistula. Acta Neurochir 141:1265–1271.
- Ono K, Arai H, Endo T, Tsunoda A, Sato K, Sakai T, Makita J. 2004. Detailed MR imaging anatomy of the abducent nerve: Evagination of CSF into Dorello canal. AJNR 25:623–626.
- Ozer E, Icke C, Arda N. 2010. Microanatomical study of the intracranial abducens nerve: Clinical interest and surgical perspective. Turk Neurosurg 20:449–456.
- Ozveren MF, Uchida K, Erol FS, Tiftikci MT, Cobanoglu B, Kawase T. 2001. Isolated abducens nerve paresis associated with incomplete Horner’s syndrome caused by petrous apex fracture—Case report and anatomical study. Neurol Med Chir 41:494–498.
- Ozveren MF, Uchida K, Aiso S, Kawase T. 2002a. Meningovenous structures of the petroclival region: Clinical importance for surgery and intravascular surgery. Neurosurgery 50:829–837.
- Ozveren MF, Uchida K, Tekdemir I, Cobanoglu B, Akdemir I, Kawase T, Deda H. 2002b. Dural and arachnoid membraneous protection of the abducens nerve at the petroclival region. Skull Base 12:181–188.
- Ozveren MF, Sam B, Akdemir I, Alkan A, Tekdemir I, Deda H. 2003. Duplication of the abducens nerve at the petroclival region: An anatomic study. Neurosurgery 52:645–652.
- Ozveren MF, Erol FS, Alkan A, Kocak A, Onal C, Tu¨re U. 2007. Microanatomical architecture of Dorello’s canal and its clinical implications. Neurosurgery 60:ONS1–ONS8.
- Piffer CR, Zorzetto NL. 1980. Course and relations of the abducens nerve. Anat Anz 147:42–46.
- Ro LS, Chen ST, Tang LM, Wei KC. 1995. Concurrent trigeminal, abducens, and facial nerve palsies presenting as false localizing signs: Case report. Neurosurgery 37:322–325. Rush JA,
- Younge BR. 1981. Paralysis of cranial nerves III, IV, and VI. Cause and prognosis in 1,000 cases. Arch Ophthalmol 99:76–79. Shi X, Han H, Zhao J, Zhou C. 2007. Microsurgical anatomy of the superior orbital fissure. Clin Anat 20:362–366.
- Takagi H, Miyasaka Y, Kuramae T, Ohwada T, Tsunoda M. 1976. Bilateral traumatic abducens nerve palsy without skull fracture or intracranial hematoma-a report of 3 cases and consideration of the mechanism of injury (author’s transl). No Shinkei Geka 4:963–969.
- Tsitsopoulos PD, Tsonidis CA, Petsas GP, Hadjiioannou PN, Njau SN, Anagnostopoulos IV. 1996. Microsurgical study of the Dorello’s canal. Skull Base Surg 6:181–185.
- Tubbs RS, Radcliff V, Shoja MM, Naftel RP, Mortazavi MM, Zurada A, Loukas M, Cohen-Gadol AA. 2011. Dorello canal revisited: An observation that potentially explains the frequency of abducens nerve injury after head injury. World Neurosurg [DOI: 10.1016/j.wneu.2011.03.046].
- Umansky F, Elidan J, Valarezo A. 1991. Dorello’s canal: A microanatomical study. J Neurosurg 75:294–298.
- Umansky F, Valarezo A, Elidan J. 1992. The microsurgical anatomy of the abducens nerve in its intracranial course. Laryngoscope 102:1285–1292.
- Yasargil MG. 2002. The internal acoustic meatus. J Neurosurg 97:1014–1017.
- Ziyal IM, Ozcan OE, Deniz E, Bozkurt G, Ismailoglu O. 2003. Early improvement of bilateral abducens nerve palsies following surgery of an anterior communicating artery aneurysm. Acta Neurochir 145:159–161.
Please login to post a comment.




