

Superior Cerebellar Artery Aneurysm



This is a preview. Check to see if you have access to the full video. Check access
Clip Ligation of a Superior Cerebellar Artery Aneurysm: Technical Principles
Aneurysms of the posterior circulation, including superior cerebellar artery (SCA) aneurysms, present unique technical challenges because they can only be accessed via maneuvering through deep operative corridors with limited working angles bounded by critical neurovascular structures.
The posterior circulation is intimately involved with the brainstem and cranial nerves, and complications related to aneurysm treatment frequently result in clinically significant consequences.
SCA aneurysms are rare lesions with a reported incidence of 1-2% of all aneurysms. The majority of these aneurysms are located at the proximal aspect of the SCA, typically at the basilar junction. The SCA supplies the main portions of the superior cerebellar hemisphere and the “roof” nuclei.
SCA aneurysms typically present with subarachnoid hemorrhage; their close association to the cranial nerves (CNs) III and IV also results in symptomatic mass effect on these nerves. The common incorporation of the proximal SCA into the neck of these aneurysms makes preservation of this parent artery challenging, and microsurgery continues to play an important role in the management of these lesions. Given the anatomic course of the SCA, surgical approaches tend to parallel the routes used to expose aneurysms of the basilar bifurcation and posterior cerebral artery (PCA).
Indications for Microsurgery
Aneurysms of the posterior circulation usually harbor a more aggressive natural history than those in the anterior circulation. Therefore, serious consideration should be given to their prompt treatment.
Factors influencing the need for treatment and choice of modality include: the patient’s age, wishes, general medical condition, and presenting symptoms; aneurysm characteristics, including size, neck-to-dome ratio, morphology, location, intraluminal thrombus, and calcification; and the experience of the practitioner. These factors are more thoroughly discussed in the Clip or Coil chapter.
Acute development of CN dysfunction related to the aneurysm requires urgent treatment of the aneurysm.
Preoperative Considerations
As discussed before, SCA aneurysms often harbor a broad neck that engulfs the origin of the SCA. A catheter arteriogram with three-dimensional (3D) reconstruction sequences is useful for defining the morphology of the neck and the surrounding vascular anatomy.
There is often a limited opportunity to thoroughly dissect the neck of ruptured SCA aneurysms because of the restricted working space provided by a swollen brain after subarachnoid hemorrhage. In addition, a complete mobilization of the aneurysm, which is often required for circumdissection of the neck, may not be safe as it can lead to premature rupture. For these reasons, it is imperative to derive as much information from the preoperative images as possible for safe placement of the clip.
The preoperative considerations for SCA aneurysms are very similar to those discussed in the Basilar Artery Bifurcation Aneurysm: Pterional Approach chapter. The altitude of the aneurysm neck in relation to the dorsum sella is an important consideration for the use of pterional versus subtemporal approach.

Figure 1: A classic SCA aneurysm is demonstrated (left). Note the relation of the neck to the origin of the SCA. Dysmorphic forms of this aneurysm are not uncommon (right).
Operative Anatomy
In the majority of patients, the SCA originates from the basilar artery, just proximal (within 2.5 mm) to the PCAs, and is the most consistent of the cerebellar arteries.
It is not unusual to see duplication of the SCA arising from the basilar artery. Other variations include a single SCA trunk derived from the proximal PCA or duplications of the SCA with the rostral trunk arising from the PCA. In addition, there are rare case reports of the SCA originating from the internal carotid artery within the cavernous sinus with no connection to the basilar artery. This morphology is believed to be a variation of a persistent trigeminal artery.

Figure 2: The operative pathway toward the right SCA is shown. Note the working space through the opticocarotid triangle. The anatomy of the SCA relative to other posterior circulation vasculature is shown (images courtesy of AL Rhoton, Jr.)

Click here to view the interactive module and related content for this image.
Figure 3: The right-sided carotid-oculomotor pathway (upper row) and the subtemporal route (lower images) are demonstrated (images courtesy of AL Rhoton, Jr.)

Click here to view the interactive module and related content for this image.
Figure 4: The subtemporal route may be extended via transection of the tentorium for low-lying SCA aneurysms (right middle image.) The trochlear nerve can be mobilized out of its dural canal within the tentorial incisura before it enters the cavernous sinus. This maneuver will expand the infratrochlear working channel (left lower image.) The anterior petrosal approach further expands the operative corridor (right lower image)(images courtesy of AL Rhoton, Jr.)
Rhoton defined the four segments of the SCA as follows: the anterior pontomesencephalic, lateral pontomesencephalic, cerebellomesencephalic, and cortical segments. I consider the anterior and lateral pontomesencephalic segments to be the proximal segments that carry vital perforating vessels to the brainstem.
The posterior thalamoperforators arise from the P1 segment of the PCA and basilar bifurcation. Although these vital vessels are often not associated with SCA aneurysms, the surgeon should take care to prevent injury to these vessels during dissection as they lie in close proximity of the aneurysm neck. Similarly, thalamogeniculate and peduncular perforators arising from the P2 segment of the PCA should be protected.
MICROSURGICAL CLIP LIGATION OF SUPERIOR CEREBELLAR ARTERY ANEURYSMS VIA THE PTERIONAL ROUTE
Aneurysms arising from the proximal SCA may be approached using the extended pterional, modified orbitozygomatic or subtemporal approaches. Less commonly considered alternatives include the combined supra- and infratentorial presigmoid transpetrosal osteotomy.
When evaluating patients for microsurgical intervention, special attention must be paid to the cranial-caudal location of the SCA aneurysm in relation to the dorsum sellae. Lesions within a 5-mm vertical span of the dorsum sellae are typically candidates for pterional or modified orbitozygomatic routes.
As the pathology descends, it becomes necessary to modify the approach to match the lesion’s location. A temporopolar transcavernous approach with resection of the posterior clinoid and drilling of the dorsum sellae may be required for lower-lying aneurysms. The modified extended subtemporal transtentorial approach is my preference in these cases. This route involves incising the tentorium just posterior to the entry site of the trochlear nerve into the tentorial incisura and releasing the nerve within its intradural canal.
The most distal segment of the SCA may be accessed using a subtemporal approach. Petrosectomy and division of the tentorium will provide a more caudal exposure. This segment can also be exposed via a retrosigmoid craniotomy—this is my preferred route.
In addition to the retrosigmoid approach, the third and fourth SCA segments can be exposed using a paramedian supracerebellar-infratentorial approach.
I prefer the pterional route when the anatomy is favorable and use the subtemporal route for low-lying SCA aneurysms. For the details of the subtemporal approach, please refer to the chapter on Basilar Artery Bifurcation Aneurysm: Subtemporal Approach.
INTRADURAL PROCEDURE
Initial Exposure
After generous dissection of the Sylvian fissure, cerebrospinal fluid should be released from the basal cisterns. The lamina terminalis can also be fenestrated early in surgery to obtain further relaxation in ruptured cases. The interpeduncular cisterns and membrane of Liliquist are split and the basilar artery bifurcation exposed to orient the operator to the local vascular anatomy.
Please review the Basilar Artery Bifurcation Aneurysm: Pterional approach chapter for more details regarding early intradural dissection and exposure of the basilar apex region.
The superior section of the basilar artery region can be exposed through one of three anatomic triangles: the opticocarotid triangle, the carotid-oculomotor triangle, or the supracarotid triangle. The carotid-oculomotor triangle is the most flexible and practical passageway to the region if the aneurysm’s vertical location along the posterior clinoid is favorable. The opticocarotid triangle is small and the supracarotid triangle is obstructed by the A1 and M1 perforating arteries.
The key to atraumatic mobilization of the frontal and temporal opercula is a robust and wide Sylvian fissure split and generous dissection of the arachnoid bands of the basal cisterns. The attachments of the oculomotor nerve to the surrounding structures are also sharply released to prevent its traction injury.
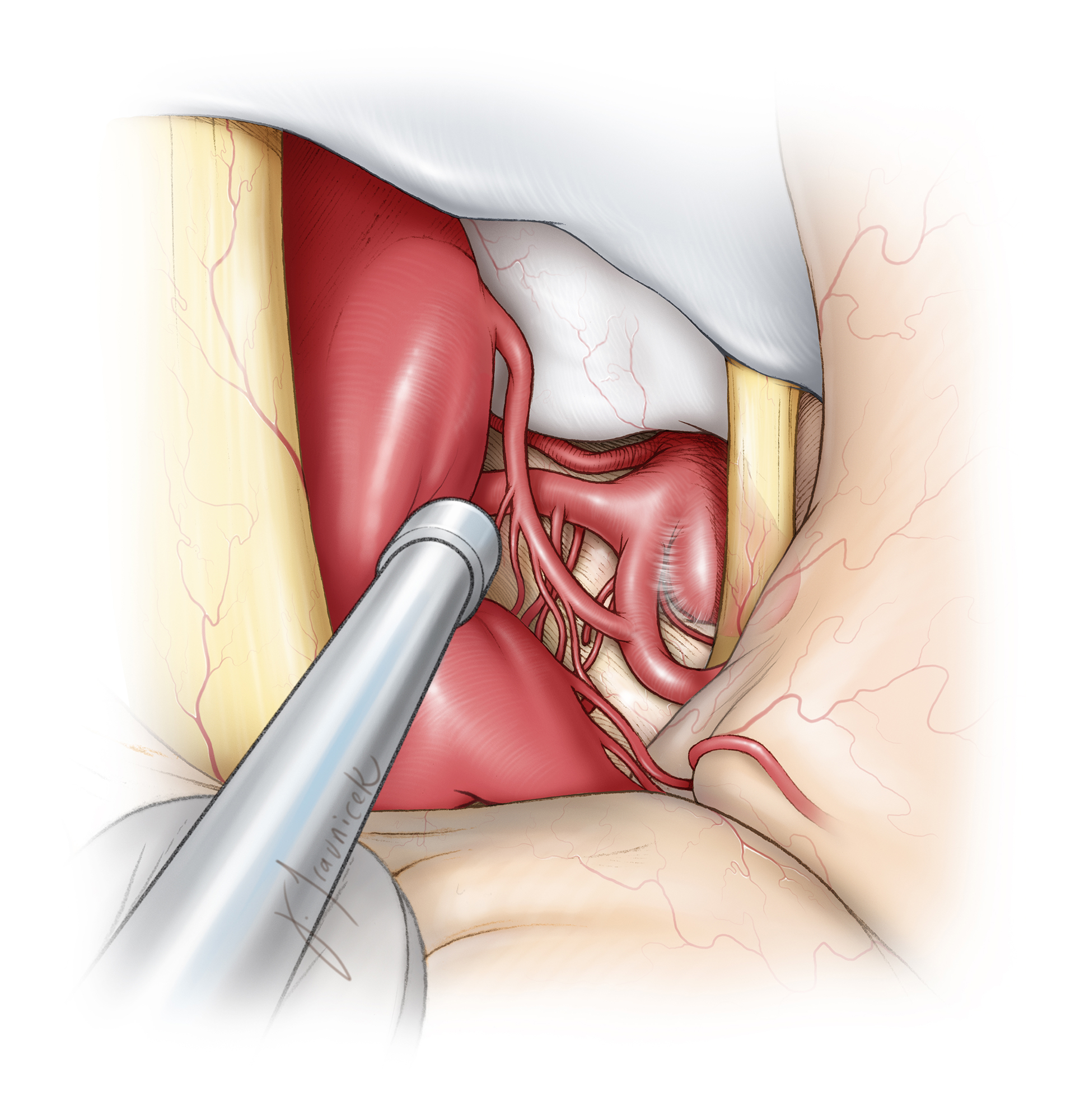
Figure 5: Once adequate brain relaxation is achieved, the posterior communicating artery (PCoA) is pursued through the carotid-oculomotor triangle, leading the operator to the P1-P2 junction. Adequate release of this artery maximizes surgical freedom within the carotid-oculomotor triangle. The thalamoperforating arteries arising from the superior aspect of the PCoA should be strictly protected and the dissection limited to its medial and inferior aspects. The oculomotor nerve is usually readily identified at this point and its relation to the SCA is carefully inspected, if the posterior clinoid is not obstructing the view of the SCA. As expected, SCA aneurysms are usually not high riding relative to the posterior clinoid.

Figure 6: A posterior clinoidectomy may be necessary to secure proximal control. The dura over this portion of the clinoid is first reflected and the clinoid is cored out using a hand drill. Once only a thin shell of bone is left behind, curettes are used to mobilize the shell. Venous bleeding from the cavernous sinus is controlled using packing of thrombin-soaked Gelfoam powder. The drill should not injure the PCoA and adjacent perforating vessels.
To decrease the turgidity of the aneurysm before its neck dissection, I place a temporary clip below the SCA’s at a perforator-free zone of the basilar trunk. The bulk of the temporary clip should not interfere with the next steps of dissection maneuvers. Unfortunately, the depth and limited working space may preclude the use of a temporary clip.
Aneurysm Dissection
Once the aneurysm neck is identified, I proceed to reliably identify the outflow vessels before aggressive neck dissection. The neck of the aneurysm is in the plane of the origins of the SCA and PCA; the fundus projects slightly anteriorly or rarely posteriorly. After defining the proximal and distal vascular anatomy, dissection of the aneurysm neck begins while the surgeon preserves the branching and perforating arteries behind and inferior to the aneurysm neck.

Figure 7: The strategic placement of the temporary clip is required so that the operative field is not compromised. I completely mobilize and circumdissect the space around the aneurysm neck. In this sketch, one of the brainstem perforators is being mobilized away from the passageway of the clips.
Suboptimal clip application and partial neck closure lead to turbulence within the sac. Blind and hasty application of a permanent clip without an adequate understanding of the neck anatomy is the most common cause of intraoperative rupture.
Preoperative imaging may be used to anticipate the appropriate clip configurations. Small SCA aneurysms are clip ligated perpendicular to the basilar artery, and a straight clip is a reasonable option.
Clip Ligation
Once the aneurysm neck is thoroughly dissected, the most practical angle of clip application is perpendicular to the axis of the basilar artery. As the clip blades are slowly closed, the tips of the blades are slightly moved away from the brainstem so that the perforating arteries behind the neck are not sacrificed. The bulky clip appliers obstruct the surgeon’s view and limit direct visualization around the neck and especially behind it during final closure of the clip blades.

Figure 8: I usually prefer a straight permanent clip to collapse the aneurysm neck. However, angled clips may improve my visualization around the neck during clip application by moving the clip appliers out of my line of sight. This clip construct also places the blades parallel to the long axis of the basilar artery and prevents distortion of the parent vessels, a potential risk associated with straight clips.
As with aneurysms in other locations, the liberal use of indocyanine green or fluorescein angiography can assist with preservation of the parent vessels and obliteration of the aneurysm. However, deep corridors compromise the quality of fluorescence imaging.
Revascularization
Proximal SCA segments whose aneurysms cannot be managed with primary clip ligation may be candidates for revascularization. In general, the SCA has even more robust collateralization than the PCA; trapping or proximal ligation is an option for management of distal SCA aneurysms.
However, the proximal SCA contains brainstem perforating arteries in more than 80% of patients. Therefore, before considering proximal ligation or trapping, I explore the aneurysmal segment for perforating arteries and I am prepared to revascularize the SCA territory.
Given the risk of cerebellar infarct and the presence of proximal perforators, I frequently plan a bypass in case the SCA is occluded. The PCA is used to revascularize the SCA territory via an end-to-side anastomosis. Many of the same donor vessels that would be candidates for PCA bypass can also be used for the SCA.
Variations
As mentioned before, the most practical method of clip application involves the use of a straight clip that is deployed perpendicular to the direction of the basilar artery. However, other clip configurations are also possible and preferred if the anatomy of the deep operative corridor is favorable.
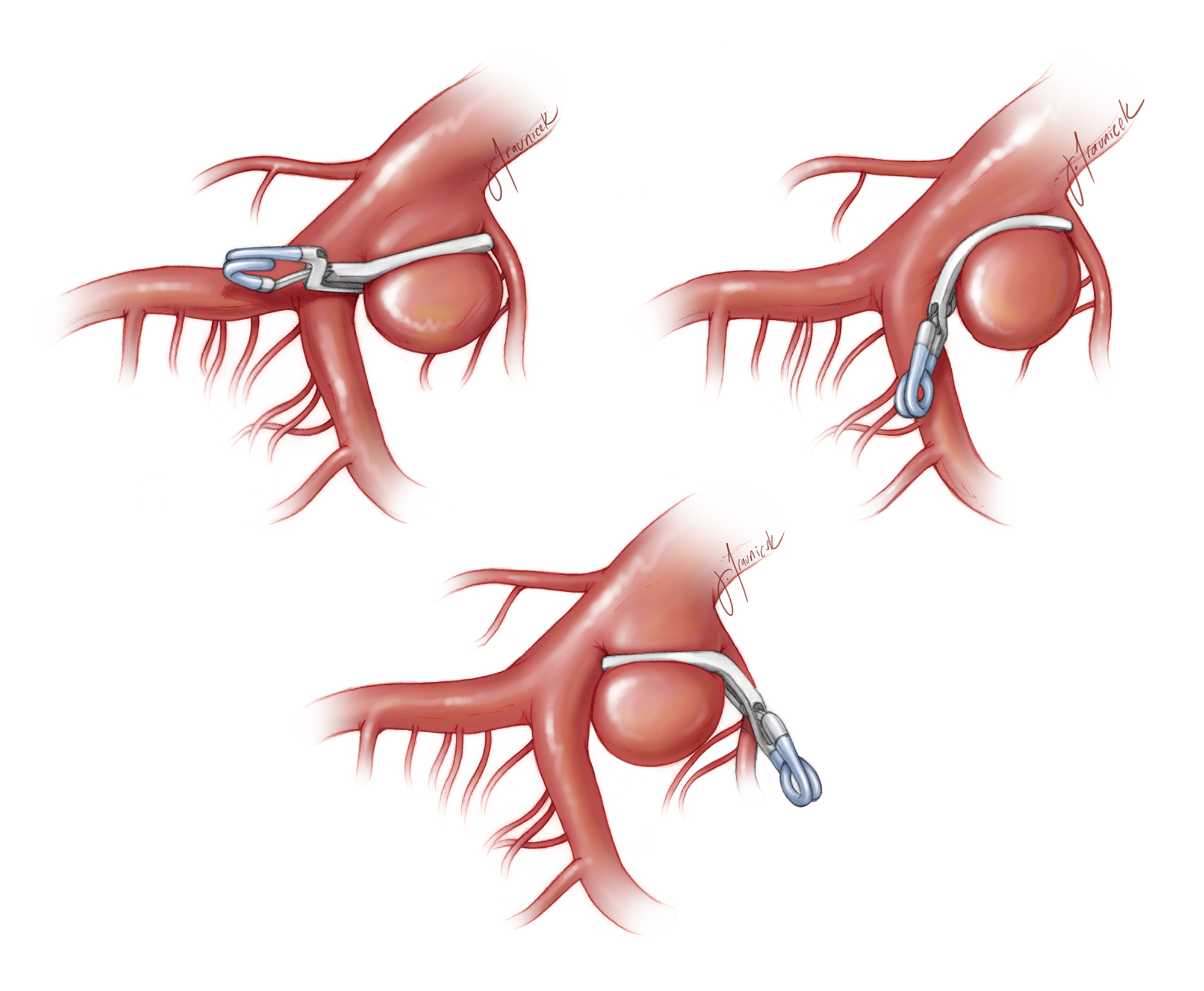
Figure 9: Three different simple clipping techniques for superior cerebellar artery aneurysms are illustrated. The aneurysm neck is clipped with a single angled clip, parallel to the afferent artery (basilar artery) from which the aneurysm arises and perpendicular to the efferent branch (left upper image); the aneurysm is more on the afferent rather than the efferent vessel. The aneurysm may also be clip ligated using a curved clip (right upper image). The curved blade allows a more desirable exclusion of the aneurysm base. If the basilar bifurcation is “high,” an angled clip may be appropriate (lower image). In the lower image, the aneurysm originates equally from both the basilar and superior cerebellar arteries.

Figure 10: A relatively classic SCA aneurysm was noted on a sagittal CTA and 3D angiogram (top row). Note the location of the aneurysm neck just below the posterior clinoid process. Proximal vascular control was expected to be a challenge and unreliable. A pterional craniotomy explored the aneurysm; the subfrontal brain was mobilized and the dome was discovered within the interpeduncular cisterns (second row, the blue arrow marks the origin of the PCA). The perforators were gently dissected away from the aneurysm neck while the aneurysm was slightly deflated via temporary inflation of a balloon endovascularly within the basilar artery. Next, an angled curved clip ligated the aneurysm effectively (third row).
Postoperative Considerations
The postoperative care of patients who have undergone clip ligation of their SCA aneurysm is not significantly different from that of other patients with cerebral aneurysms. Blood pressure control on the eve of surgery is necessary to minimize the risk of a postoperative hematoma. Temporary third nerve palsy is not uncommon and usually resolves within 6 weeks.
Pearls and Pitfalls
- The anatomy of the interpeduncular cisterns is complex and should not be taken for granted. More than one anatomic landmark should be used for reliable intraoperative orientation.
- I recommend dissection of most basilar apex aneurysms under brief periods of proximal temporary occlusion.
- Each perforating vessel of the basilar apex territory carries life through it. Meticulous dissection of the neck and perforator preservation cannot be overemphasized.
Contributors: Jonathan Russin, MD, and Yashar Kalani, MD
References
Batjer HH. Aneurysms of the superior cerebellar artery, in Samson DM (ed): Intracranial Aneurysm Surgery: Techniques. Mount Kisco, NY: Future Publishing, 1990.
Russin J, Spetzler RF. Microsurgical management of aneurysms of the posterior cerebral, superior cerebellar and anterior inferior cerebellar arteries, in Spetzler RF, Kalani MY, Nakaji P (eds): Neurovascular Surgery. New York: Thieme, 2015.
Related Materials
Available Through the Atlas
-
Microsurgical management of aneurysms of the superior cerebellar...
-
Clipping of ipsilateral posterior communicating and superior cere...
-

Management-related morbidity in unselected aneurysms of the upper...
Unavailable Through the Atlas
Please login to post a comment.



