

Skull Fractures


Figure 1: Axial CT through the skull base demonstrates linear lucency through the greater wing of the left sphenoid bone representing a simple nondisplaced fracture. Small nondisplaced fractures can also mimic suture lines. Careful attention to symmetry and review of an anatomic atlas may aid in differentiating the two.

Figure 2: CT on bone window (top row left) clearly demonstrates a depressed right calvarial fracture with override of the fragments. Low density foci of scalp soft tissue emphysema and pneumocephalus are also visible. CT on brain window in the same patient makes the left subdural hematoma much more clearly visible. Midline shift is also present indicating subfalcine herniation (top row right). The basal cisterns are also effaced in this patient (bottom row), indicating the degree of mass effect from edema and hematoma.

Figure 3: Coronal CT views of the upper cervical spine is often the best way to detect type III occipital condyle fracture, an unstable injury due to avulsion of the alar ligament.
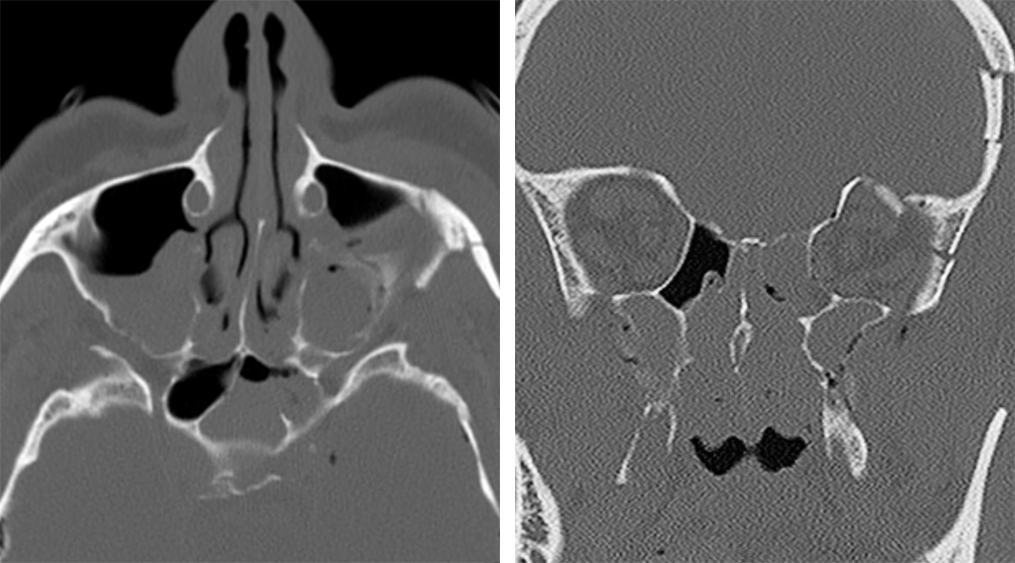
Figure 4: Comminuted fractures traverse the orbital and paranasal sinus walls on this coronal CT of the maxillofacial area (left). The fracture lines also involve the sphenoid bone and fovea ethmoidalis (roof of the ethmoid air cells). Axial images (right) demonstrate layering material in the maxillary and left sphenoid sinuses representing blood and possibly CSF, given the patient’s elevated risk related to the fracture pattern.
- Can be asymptomatic
- Can cause serious injury to vessels (arteries, veins, and dural venous sinuses), cranial nerves and the underlying brain
- Morphology can be simple, comminuted, linear, depressed or elevated, overriding, and closed or open
- Middle cranial fossa is the weakest with thin bones and multiple foramina and is more prone to fracture
Neuroimaging
- Skull Radiograph
- Non-preferred modality to evaluate a fracture
- Fracture visualized as a linear calvarial lucency
- Very few non-displaced fractures are better visible on radiographs than on CT
- CT Angiogram is used to evaluate for associated vascular injury
- CT findings
- Primary tool for evaluation of skull fractures
- Scout view can act as a radiograph to increase the sensitivity for horizontally oriented skull fractures
- Linear fracture
- Sharply delineated lucent line (See Figure 1; for additional illustrations reference the Epidural Hematoma chapter)
- May have overlying scalp edema and underlying extra-axial hematoma
- Depressed fracture (See Figure 2)
- Fracture with inward displacement of the fractured fragment; which is usually palpable
- Often associated with extra-axial hemorrhage
- May see underlying dural venous sinus compromise
- More likely associated with underlying brain contusion
- Skull base fracture
- Can cause pneumocephalus and air within TMJ glenoid fossa
- May cause air-fluid level within adjacent mastoid air cells or paranasal sinuses that clinically presents with CSF rhinorrhea, CSF otorrhea, hemotympanum
- When involving the temporal bones:
- 70-90% are longitudinal; these present with conductive hearing loss
- 20 – 30% are transverse; these present with neurosensory hearing loss (Holland BA, Brant-zawadzki M. High-resolution CT of temporal bone trauma. AJR Am J Roentgenol. 1984;143 (2): 391-5)
- Occipital condylar fracture (See Figure 3)
- Avulsion injury at the site of alar ligament attachment
- Best seen on coronal CT images
- Associated clinical symptoms include coma, associated cervical spinal injuries, lower CN deficits, hemiplegia, quadriplegia, Collet-Sicard syndrome (CN 9, 10, 11, 12 deficits)
- Sphenoid bone fracture
- May cause CSF leak (See Figure 4)
- MRI findings
- MRI is obtained in complicated cases
- T2 weighted imaging delineates dural injury
- FLAIR helps delineate cerebral contusion, which shows up as hyperintense signal
- T2*/GRE/SWI identifies foci of hemorrhage susceptibility
- MR Angiogram detects arterial injury
- MR Venogram detects venous injury
- Differential Diagnoses for fracture
- Suture line
- Vascular groove
- Arachnoid granulation
- Venous lake
For more information, please see the corresponding chapter in Radiopaedia.
Contributor: Priya Rajagopalan, MD
Please login to post a comment.




