

Colloid Cyst

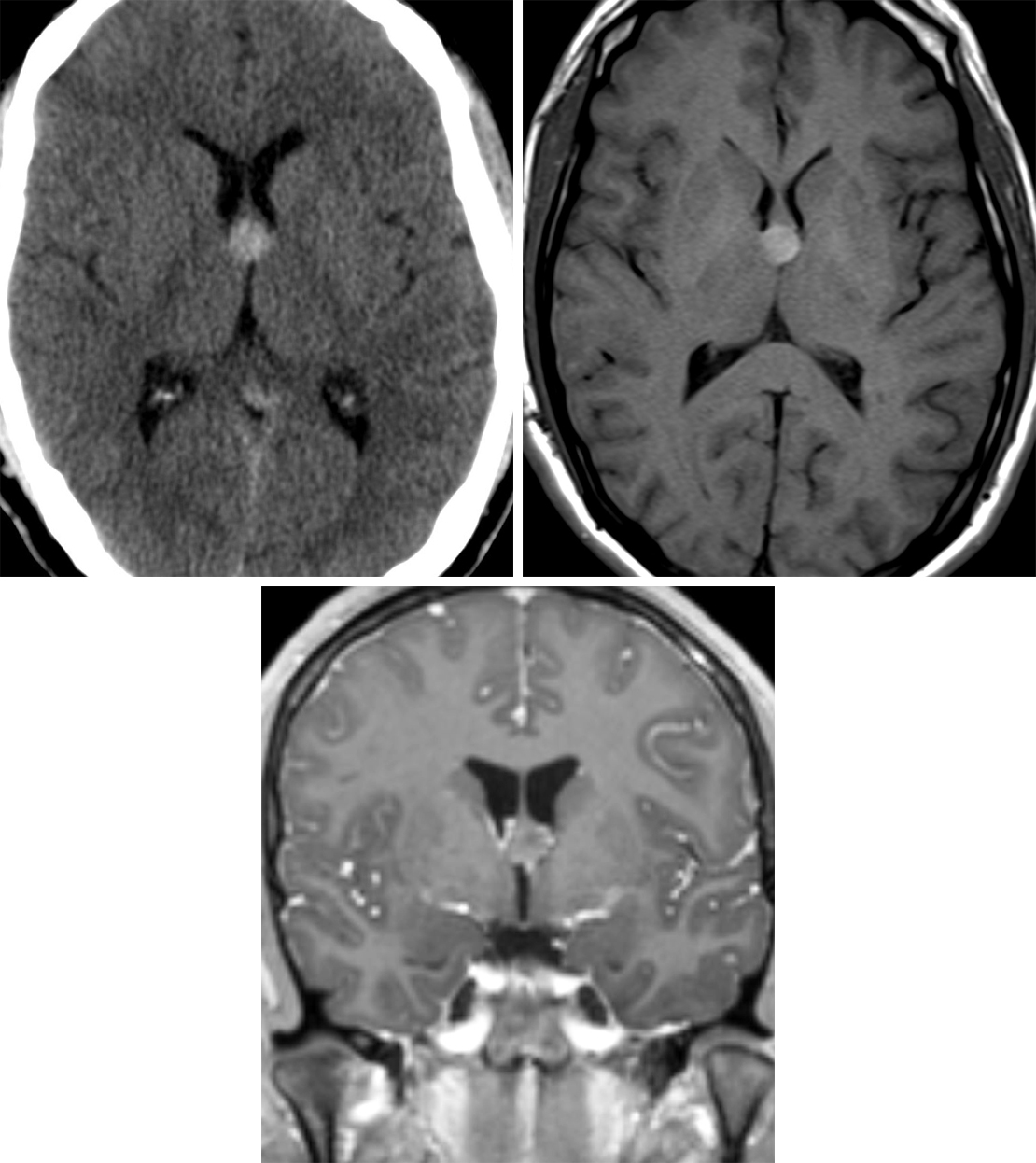
Figure 1: Because colloid cysts are typically filled with a highly proteinaceous fluid, they are often dense on CT (top left) and hyperintense on T1-weighted (top right) imaging. (Bottom) Colloid cysts should have no internal enhancement on T1-weighted postcontrast imaging. This colloid cyst is in the classic location at the foramen of Monro.
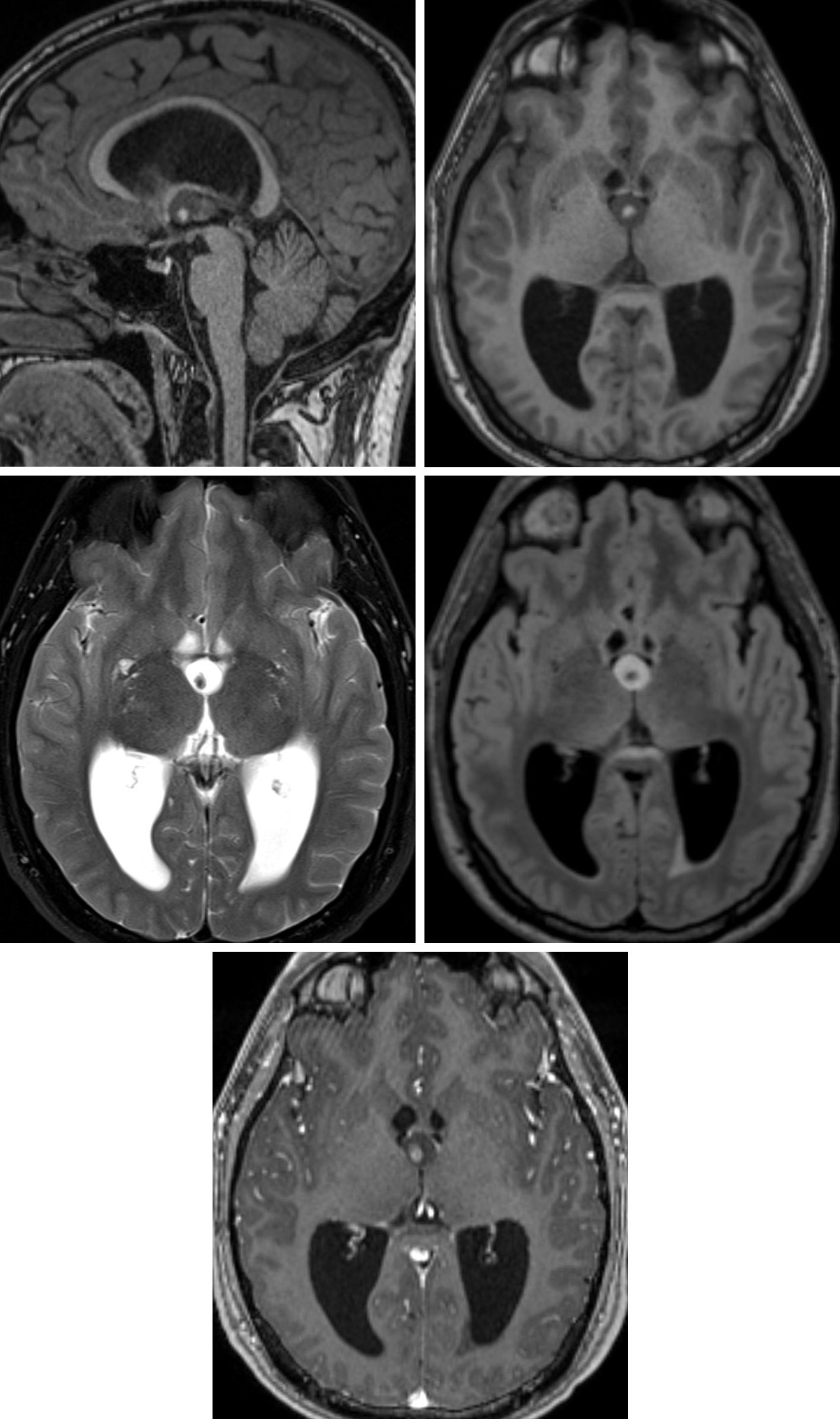
Figure 2: Sagittal (top left) and axial (top right) T1-weighted images demonstrate a low-signal-intensity colloid cyst at the foramen of Monro. The cyst has a central T1 hyperintense focus that represents inspissated proteinaceous debris. (Middle Left) The cyst is bright on T2 with low-signal-intensity proteinaceous debris that is sometimes referred to as the “black hole” effect. (Middle Right) The cyst remains predominantly hyperintense on FLAIR imaging, indicating its content dissimilarity from CSF. (Bottom) This cyst has no appreciable enhancement on postcontrast imaging, with its only hyperintense component being the intrinsically T1 hyperintense debris centrally. Obstructive hydrocephalus is present on these images, a known common risk of colloid cyst due to their position. Incidentally, the internal proteinaceous debris is mobile in this cyst, indicated by its change from a central position on the earlier sequences (top left, top right, and middle right) to a right posterior position on the later sequences (middle left and bottom).
BASIC DESCRIPTION
- Mucin-containing unilocular third-ventricular cyst often located near the foramen of Monro
- Synonymous terms: paraphyseal or neuroendodermal cyst
PATHOLOGY
- Congenital abnormality due to ependymal encystment or persistence of the paraphysis
- Thin fibrous capsule of simple or pseudostratified epithelium with goblet and ciliated cells
- Center filled with mucin, cholesterol, and desquamated epithelium
CLINICAL FEATURES
- Most common during third and fouth decades of life
- Uncommon in children
- No gender predilection
- Majority are stable in size and without ventricular obstruction
- Minority continue to enlarge, causing intraventricular obstructive hydrocephalus ± coma, death
- Common presenting signs/symptoms
- Small cysts: positional headache
- Larger obstructing cysts: sudden-onset hydrocephalus with herniation, coma, and sudden death
- Treatment: surgical resection, cerebrospinal fluid (CSF) shunting
IMAGING FEATURES
- General
- Well-marginated hyperdense unilocular cyst arising within anterior third ventricle near the foramen on Monro (99%)
- Forniceal pillars elevated over cyst
- Size variable
- ±Hydrocephalus
- CT
- Majority are hyperdense due to high proteinaceous content
- No enhancement on contrast-enhanced CT imaging
- MRI
- T1WI: isointense to hyperintense due to cholesterol content
- T2WI: variable signal intensity
- FLAIR: hyperintense
- DWI: no diffusion restriction
- T1WI+C: no enhancement
IMAGING RECOMMENDATIONS
- Nonenhanced head CT, MRI without and with intravenous contrast (to exclude mimics); serial imaging follow-up for small cysts without hydrocephalus
For more information, please see the corresponding chapter in Radiopaedia.
Contributor: Rachel Seltman, MD
References
Demirci S, Dogan KH, Erkol Z, et al. Sudden death due to a colloid cyst of the third ventricle: report of three cases with a special sign at autopsy. Forensic Sci Int 2009;189:e33–e36. doi.org/10.1016/j.forsciint.2009.04.016.
El Khoury C, Brugières P, Decq P, et al. Colloid cysts of the third ventricle: are MR imaging patterns predictive of difficulty with percutaneous treatment? AJNR Am J Neuroradiol 200021:489–492.
Osborn AG, Salzman KL, Jhaveri MD. Diagnostic Imaging (3rd ed). Elsevier, Philadelphia, PA; 2016.
Sheikh AB, Mendelson ZS, Liu JK. Endoscopic versus microsurgical resection of colloid cysts: a systematic review and meta-analysis of 1,278 patients. World Neurosurg 2014;82:1187–1197. doi.org/10.1016/j.wneu.2014.06.024.
Please login to post a comment.




