

Parietal Craniotomy Free



General Considerations and Operative Anatomy
Parietal craniotomy is designed to provide an operative exposure of the mid to posterior hemisphere while sparing the highly functional anteriorly located sensorimotor cortices and the posteriorly located visual cortex. The approach can be devised to lateral and mesial parietal lobe lesions as well as to interhemispheric median or paramedian lesions.
The variations of this corridor allow access to lesions through the transcortical route (through the more functionally “silent” superior parietal lobule) or the interhemispheric fissure. The parasagittal veins are often less numerous in the posterior parietal region, therefore providing an opportunity to reach deep lesions through the interhemispheric trajectory.
The right or nondominant parietal lobe (see Wikipedia) is implicated in spatial awareness and navigation. Operative interventions that place the entire right lobe at risk are associated with hemibody neglect. This neglect does significantly improve over time, but some residual disability persists.
The left or dominant parietal lobe (see Wikipedia) is involved in symbolic functions in language and mathematics. Damage to the left lobe results in problems with mathematics, long reading, writing, and understanding symbols. Gerstmann's syndrome is associated with lesions in the dominant inferior parietal lobe, whereas Balint's syndrome (simultanagnosia, oculomotor apraxia, optic ataxia) is associated with bilateral lesions.
The posterior parietal cortex can be subdivided into the superior parietal lobule (Brodmann areas 5 + 7) and the inferior parietal lobule (39 + 40), separated by the intraparietal sulcus.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features

Click here to view the interactive module and related content for this image.
Figure 1: Lateral (A), anterior (B), and posterior (C) views of the cerebrum. Note the location of the superior and inferior parietal lobules separated by the intraparietal sulcus (C). Parasagittal bridging veins are variable in their size and location and play an important role in draining the paramedian hemispheres. Venous lakes along the superior sagittal sinus can be problematic if the dural opening is extended close to the midline (B)(Images courtesy of AL Rhoton, Jr).
Parietal lobe veins are classified according to surface of drainage (medial or lateral group) and to the direction of drainage (ascending group: drain to the superior sagittal sinus or descending group: drain to the inferior sagittal sinus or the sylvian fissure). On the lateral surface of the lobe, the ascending veins are the central, postcentral, anterior and posterior parietal veins, while parietosylvian veins form the descending group. On the medial surface of the lobe, the ascending veins are the paracentral, anteromedial and posteriomedial parietal veins. Finally, the descending group is formed by the posterior pericallosal veins.
The lateral group also includes the vein of Trolard, also known as superior anastomotic vein, which crosses the frontal and parietal lobes on its way from the sylvian fissure to the superior sagittal sinus. The most common location of the vein of Trolard is the postcentral region, but it can also be found at the central or precentral region. The cortical veins drain directly to the superior sagittal sinus or may join a parasagittal meningeal sinus or lacunae in the dura, which is the drainage channel of meningeal veins commonly located at the parietal and posterior frontal areas.

Figure 2: Superior (upper left), oblique (upper right) and posterior views (lower row) of the cerebrum demonstrating the ascending group of veins that drain the parietal lobe (central, postcentral, anterior and posterior parietal veins). Ant.: anterior; Cent.: central; Mid.: middle; Front.: frontal; Par.: parietal; Post.: posterior; Sag.: sagittal; Str.: straight; Sup.: superior; Temp.: temporal; V.: vein. (Modified with permission, courtesy of AL Rhoton, Jr.)
Indications for the Approach
The parietal craniotomy is used for both intra- and extra-axial lesions of the region, including neoplasms such as metastases, gliomas, and meningiomas, and vascular lesions such as arteriovenous malformations and cavernous malformations. The parietal interhemispheric corridor is used to approach parafalcine, medial parietal, and splenial lesions.
The parietal craniotomy is most often performed for convexity, falcine, and parafalcine meningiomas. In these cases, the patent superior sagittal sinus and the associated draining veins are at risk and should be spared to avoid disabling venous infarcts. Any dissection around the tumor capsule should protect en passage veins and arteries. As discussed above, vascular injuries in the parietal lobe can cause deficits in spatial awareness, sensorimotor function, and visual processing, and also risk injury to the nearby motor cortex and deep white matter tracts.
Parietal craniotomy can also be used to approach paramedian (periatrial) lesions of the atrium of the lateral ventricle. The traditional approach to the atrium involves a transcortical route through the superior parietal lobule with a risk of deficits in spatial awareness such as astereognosia and speech or visual processing. Recent studies have suggested that, depending on the patient’s occupation and activities, quality of life may indeed be significantly impacted by such deficits.
To avoid these risks, lesions of the atrium can be approached through a paramedian posterior parietal craniotomy and contralateral interhemispheric transfalcine approach through the precuneus. This approach provides a longer and more technically challenging path to the atrium, but involves less white matter tract disruption and brain retraction.
Preoperative Considerations
Cortical stimulation mapping under “awake,” “sleep” conditions or phase reversal mapping may be considered for localizing the sensorimotor cortex for intraparenchymal lesions situated along the anterior parietal area. Since early access to the basal cisterns is not available during parietal craniotomies, I have a low threshold for placing a lumbar drain, even for large lesions with significant mass effect. To avoid transtentorial herniation in the case of massive lesions with midline shift, I open the drain to remove cerebrospinal fluid (CSF) during dural opening. This CSF drainage significantly assists with brain relaxation and manipulation of edematous brain.
If the interhemispheric corridor is considered and large parasagittal veins are suspected on preoperative contrast-enhanced magnetic resonance (MR) imaging, an MR or CT venogram guides the location of craniotomy. The venogram will also confirm the patency of the superior sagittal sinus in the presence of an infiltrating meningioma. If numerous parasagittal veins prohibit the ipsilateral interhemispheric corridor, the contralateral interhemispheric transfalcine route may be considered for parafalcine lesions.
Transfalcine Route for Preservation of Parasagittal Veins
If the tumor partially infiltrates the lumen of the venous sinus and the risk of air embolism is significant, a preoperative cardiac diagnostic workup is necessary to exclude the risk of a paradoxical air embolism. A transesophageal echocardiogram and transthoracic Doppler may be used and there should be a low threshold of suspicion for air embolism during the procedure.
PARIETAL CRANIOTOMY

Figure 3: The patient is positioned three-quarters prone on the operating room table. This position precludes the need to turn the patient’s head into a nonphysiologic posture, as would be the case if the patient were positioned supine. Moreover, the lateral position promotes the extra-axial lesions to remain readily accessible and gravity retraction can be exploited for reaching the interhemispheric fissure. The patient must be firmly secured to the table because tilting the table during surgery can risk patient displacement.
The degrees of the patient’s head turn and tilt are dependent on the exact location of the lesion with respect to the midline, coronal, and lambdoid sutures. For parafalcine parietal lesions, the side of the lesion can be placed in the dependent position to use gravity retraction while tilting the head away from the floor to permit a more ergonomic sitting position for the operator during microsurgery. Similarly, when approaching the atrium or periatrial region through the contralateral transfalcine route, I prefer to place the patient in a three-quarters prone position and the normal hemisphere on the dependent side.
An axillary roll supports the contralateral axilla. The ipsilateral shoulder is gently pulled anteriorly and inferiorly and secured with tape to keep it out of the operator’s working zone. For convexity lesions, it is advantageous to tilt the patient’s head enough to place the lesion at the highest point in the operative field.

Figure 4: The patient’s head is secured in a skull clamp. The application of a skull clamp should satisfy certain principles. First, a line connecting the single pin with the midpoint between the opposite two pins (swivel rocker arm) must cross the equator of the patient’s head to prevent skull clamp fixation failure and head slippage. Second, the pins should not be placed close to the vertex. This positioning of the head will allow the gravity to retract the dependent hemisphere and facilitate a more expanded corridor through the interhemispheric trajectory. This head position is in contrast to the position in the next sketch where a cortical or convexity lesion is exposed and the lesion is placed close to the highest point of the operative field.
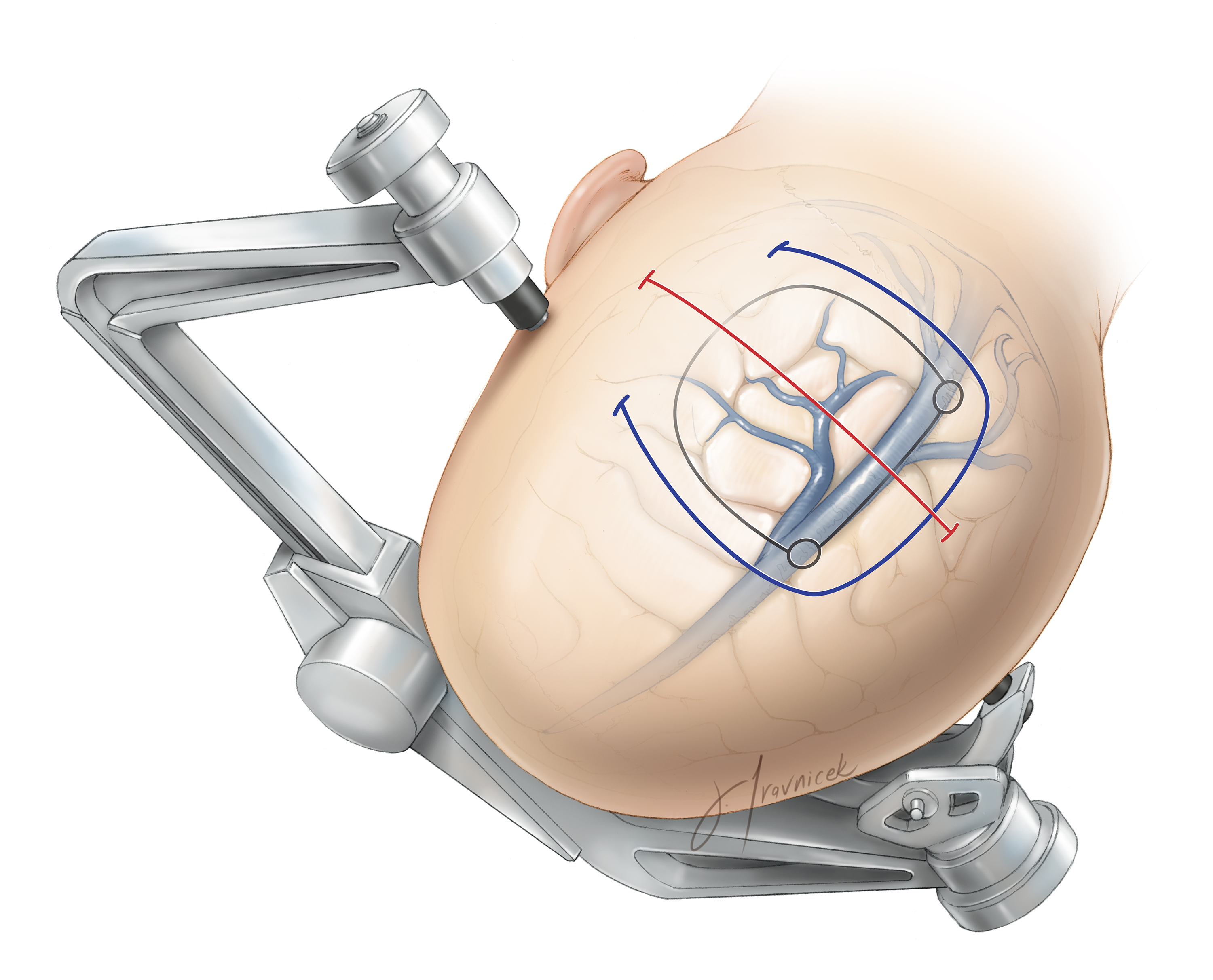
Figure 5: Various incision styles have been marked. The linear incision (red) often provides ample exposure. The horseshoe incision (blue) is reserved for large convexity meningiomas. The paramedian craniotomy is outlined (black). I use neuronavigation or preoperative MR venogram/angiograms to position the craniotomy. This tool assists with localizing and avoiding parasagittal bridging veins, especially for procedures requiring interhemispheric dissection.

Figure 6: For large lateral convexity meningiomas and gliomas, a traditional horse shoe incision is reasonable. The head is rotated until the lesion is placed at the summit of the operative field.

Figure 7: For paramedian interhemispheric lesions, I place two burr holes over the superior sagittal sinus as guided by neuronavigation. The sinus is typically deviated to the right of the sagittal suture in most patients; the maximum deviation is usually no more than 11 mm. Early identification of the sinus helps me plan the size and location of the bone flap.
A Penfield #3 dissector is used to generously dissect between the inner table of the calvarium and the wall of the superior sagittal sinus. If the wall of the sinus is adherent, a third burr hole should be placed; all burr holes should be readily in continuity within the epidural space. Cerebrospinal fluid drainage through the lumbar drain mobilizes the wall of the venous sinus and the dura away from the bone, therefore preventing their injury by the footplate of the drill. The last bony cut should be made over the venous sinus. This maneuver allows a timely elevation of the bone flap if bleeding is encountered and an injury to the sinus has occured.
Upon elevation of the bone flap, mild to moderate bleeding from the sinus wall may be controlled with thrombin-soaked gelfoam or SURGICEL Fibrillar (Somerville, NJ). The latter is left in place untouched during closure. Please refer to the chapter on the Repair of Dural Venous Sinus Injury in the Principles of Cranial Surgery Volume for further details regarding managing injuries to the sinus.

Figure 8: For convexity or intraparenchymal lesions, the dura is opened circumferentially around the tumor with a 2-cm margin away from the contrast-enhancing region as guided by intraoperative navigation (left image).
If I plan to reach the interhemispheric space (right image), I open the dura in a curvilinear fashion and create a dural flap based on the superior sagittal sinus. Care is taken to avoid injuring the large draining veins. Occasionally, a small draining vein may need to be sacrificed. If a parasagittal vein is encountered draining into the sinus, the dural opening must be adjusted to protect the vein’s inlet into the sinus (left image, inset).
Note that the bridging veins move in the posterior-to-anterior direction to drain into the sinus and may have multiple tributaries. Paramedian extensions of the superior sagittal sinus or venous lakes are frequently encountered in this region. Their presence may limit opening the dura close to the midline and restrict the interhemispheric exposure. In this situation, the dural incision near the midline may be extended parallel rather than perpendicular to the venous sinus.
Because of unpredictable lateral reach of the venous lakes, a small tear along the lateral wall of the sinus can be encountered during the paramedian dural incision. The tear should be closed using fine sutures. Bipolar coagulation leads to shrinkage of the dura and expansion of the tear.

Figure 9: To reach the parafalcine space, I release the veins through their arachnoid adhesions and untether them in preparation for their mobilization. This maneuver may be tedious because the arachnoid membranes can be thick and highly adherent. CSF lumbar drainage affords early mobilization of the hemisphere away from the midline and falx (left image).
I place retraction sutures within the superior falx and gently mobilize and rotate the superior sagittal sinus, thereby expanding the operative corridor and working angles within the interhemispheric space (right image).

Figure 10: The next steps of microdissection within the interhemispheric corridor can now begin. The parasagittal veins should not be placed under significant tension.
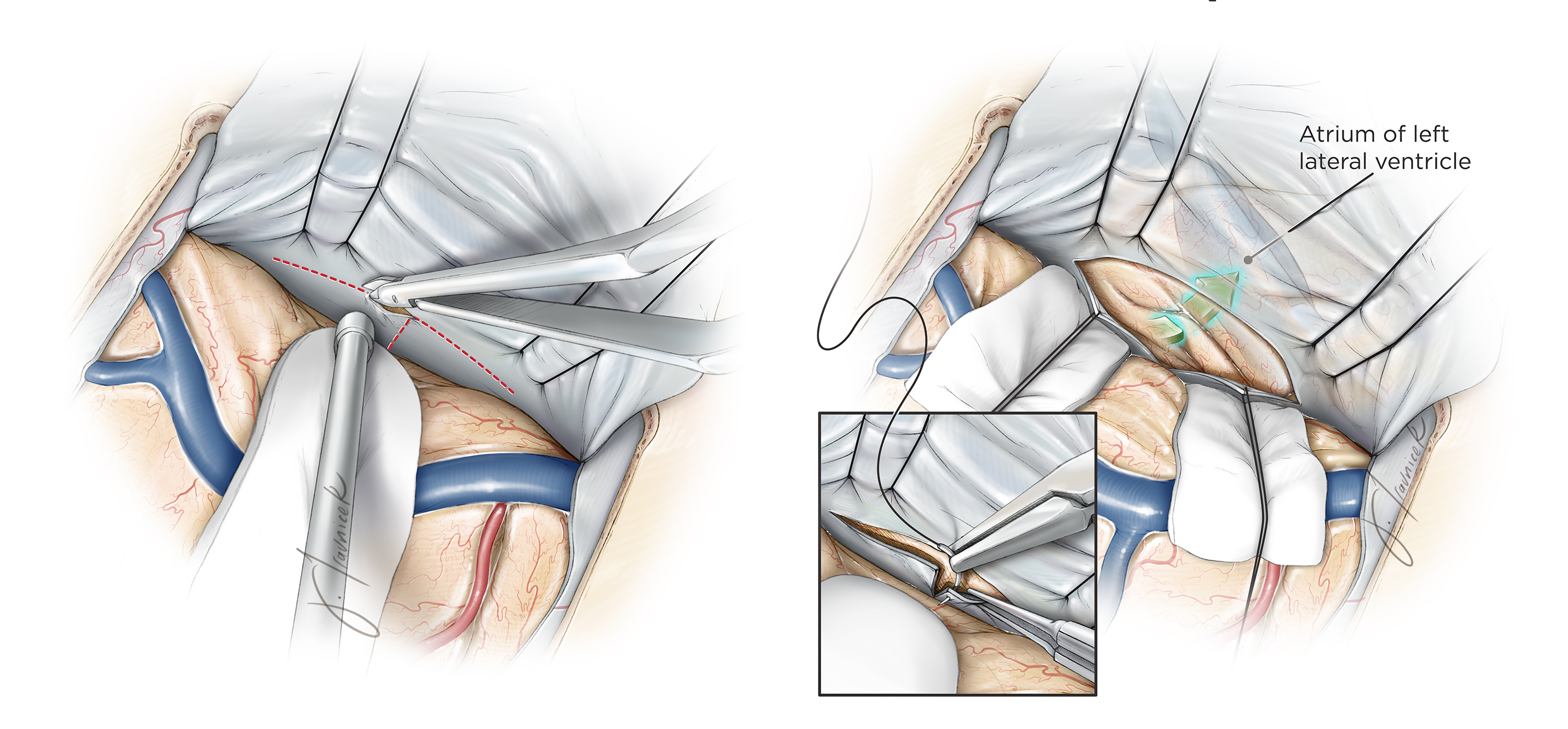
Figure 11: To reach the contralateral periatrial region, I create a T-shaped incision within the falx (left image). The falcine flaps are reflected and held in place with retraction sutures. A corticotomy through the contralateral precuneus and oblique white matter dissection within the medial contralateral hemisphere allow entry into the atrium (green arrow, right image). Division of the falx, cortex, and white matter are performed using navigation.
Peri-atrial Meningioma: Transfalcine Approach
Closure
Once the pathology is handled, hemostasis is achieved and the surgeon’s attention turns to closure. If the ventricle is entered, a ventricular drainage catheter may be placed to clear debris within the ventricles during the immediate postoperative period.
I do not routinely close the dura in a watertight fashion for supratentorial craniotomies. I avoid allograft dural substitutes for their risk of aseptic inflammation or infection. Dural closure should not “kink” or compromise flow within the parasagittal veins.
Pearls and Pitfalls
- The three-quarters prone position is a reasonable option for parietal lesions as it facilitates access to the ipsilateral lesion and allows gravity retraction to expand the interhemispheric operative corridor.
- Injury to the superior sagittal sinus during a paramedian craniotomy should be prevented at all costs. Keep a low threshold of suspicion for air embolism.
- Parasagittal bridging veins often do not receive the respect they deserve. A venous infarction in this region can be catastrophic.
Contributor: Marcus A. Acioly, MD, PhD
References
Al-Mefty O. Operative Atlas of Meningiomas. Philadelphia: Lippincott-Raven, 1998.
Alvernia JE, Lanzino G, Melgar M, Sindou MP, Mertens P. Is exposure of the superior sagittal sinus necessary in the interhemispheric approach? Neurosurgery. 2009;65(5):962-965.
Raza S, Quinones-Hinojosa A, Olivi A. Convexity meningiomas, in DeMonte F, McDermott M, Al-Mefty O (eds): Al-Mefty’s Meningiomas, 2nd ed. New York: Thieme Medical Publishers, 2011.
Rhoton AL Jr: The cerebrum. Neurosurgery. 2002;51(Suppl 1): S1-51.
Rhoton AL Jr. The cerebral veins. Neurosurgery. 2002;51(4 Suppl):S159-205.
Steinmet M, Krishnaney A, Lee J. Surgical management of convexity ,eningiomas In Badie B. (ed): Neurosurgical Operative Atlas: Neuro-oncology, 2nd ed. Rolling Meadows, IL: Thieme Medical Publishers and the American Association of Neurological Surgeons, 2007.
Tew JM Jr, van Loveren HR. Atlas of Operative Microneurosurgery, Vol 1. Philadelphia: Saunders, 1994.
Tew JM Jr, van Loveren HR, Keller JT. Atlas of Operative Microneurosurgery, Vol 2. Philadelphia: Saunders, 2001.
Please login to post a comment.





Comments: