

Frontal Lobectomy



This is a preview. Check to see if you have access to the full video. Check access
Principle Techniques for Frontal Lobectomy
The estimated prevalence of epilepsy in North America is 5 to 10 cases per 1,000 people. It is also estimated that approximately one-third of patients with epilepsy fail to achieve adequate seizure control by means of antiepileptic drugs or are unable to tolerate the side effects required to do so. A large body of evidence indicates that failing to adequately control seizures impairs cognition, decreases overall quality of life, and increases mortality compared with age-matched controls.
Medical intervention is the first step in treating epilepsy. Despite treatment with various antiepileptic drugs, medical therapy fails to achieve seizure freedom in up to one-third of patients. In a subset of patients who do not respond to medical therapy, surgical evaluation is appropriate. Approximately 5 to 10% of the population with epilepsy have uncontrolled seizures. This translates to 100,000 patients with epilepsy in the United States who are potential surgical candidates, with an additional 5,000 to 10,000 patients added annually; however, only a small fraction of this population actually are thoroughly evaluated and ultimately undergo epilepsy surgery.
For patients with medically intractable epilepsy, the probability of responding to each successive antiepileptic drug (AED) is lower with every additional AED attempted. The success rate of the first attempt with an AED is 70%, and the success rate declines to 40% with the second AED if the first attempt was unsuccessful. In addition, the percentage of patients that respond to three or more medication attempts is marginal at best. Seizure control in such patients is highly unlikely and they tend to suffer from the adverse effects of AEDs.
The interest in extratemporal epilepsy surgery has grown over the past several decades because of new imaging modalities and technologic advances in electroencephalography (EEG) and, more specifically, invasive intracranial monitoring.
Additionally, there have been numerous studies that have further described the surgically remediable syndromes for which long-term outcomes have been validated. This chapter outlines the modalities used for diagnosis and evaluation of extratemporal epilepsy and more specifically frontal lobe epilepsy (FLE), my surgical approach to FLE, and outcomes after surgery.

ATLAS Choice Bipolar Forceps
Designed for your every surgical maneuver
Five tip sizes for brain and spine procedures
Unparalleled non-stick and low-profile features
Diagnosis and Evaluation of Frontal Lobe Epilepsy
History and Physical Examination
The comprehensive preoperative assessment always includes a detailed history and physical exam. Seizure semiology, medical history, family history, and details about attempted antiepileptic medications should be included. It is often useful to have a family member or friend present who has witnessed seizure episodes because the patient may have difficulty recalling events. A complete neurologic examination, in conjunction with the history, may help identify and approximate the seizure focus.
General characteristics of frontal lobe seizures include prominence of motor manifestations, rapid secondary generalization, focal clonic motor activity (with or without march), prominent asymmetric tonic posturing, complex or bizarre motor automatisms, explosive onset and sudden cessation without postictal confusion, frequent/brief seizures in clusters, and status epilepticus of all types.
There are several clinically recognized frontal lobe seizure types, including supplemental motor area seizures, cingulate seizures, anterior frontopolar seizures, orbitofrontal seizures, dorsolateral seizures, opercular seizures, and motor cortex seizures.
Although the above classification is useful, seizures of different origins often present with nonclassical and overlapping clinical manifestations due to their rapid spread, making reliable localization of the seizure onset nearly impossible without EEG or imaging correlation. Furthermore, similar clinical seizure patterns may result from rapid seizure spread from other regions of the brain into the frontal lobe.
Despite the challenges of restricting certain ictal semiologic features to particular frontal lobe regions, some general trends do exist that may help with localization. Generalized tonic-clonic convulsions typically are associated with seizures involving the dorsolateral frontal lobe. If seizures are asymmetric/tonic, then the supplemental motor area or medial frontal areas can be implicated. Seizures with an absence component implicate the cingulate gyrus and medial frontal lobe. Motor and clonic seizures typically originate from the peri-rolandic area. Sudden motor arrest seizures may occur in all types of frontal lobe seizure categories.
Interictal Electroencephalography
Frontal lobe seizures can have complex and widely variable epileptiform abnormalities that present on EEG. Interictal EEG can also be useful in determination of the anatomic origin of the seizure, but its role is more limited in frontal lobe epilepsy than temporal lobe epilepsy.
Approximately 70% of patients with frontal lobe seizures have interictal discharges, but most are generalized, multifocal, or poorly localized. Additionally, much of the frontal lobe cortex is inaccessible to routine EEG recordings. Several cortical areas, including the orbital, mesial interhemispheric, and cingular cortices, are immeasurable with extracranial electrodes.
Many patients with frontal lobe epilepsy may show regional and multilobar distribution of ictal spikes and onset. This may be due to functional networks and pathways within the frontal and temporal lobes connected via the uncinate fasciculus and cingulum. For this reason, patients with a unilateral frontal lobe epilepsy focus may exhibit bifrontal or generalized spike and wave activity. Despite these shortcomings of EEG for frontal lobe epilepsy, when combined with modern imaging technologies and video EEG, initial evaluation of patients with medically intractable epilepsy is often very contributory.
Video Electroencephalography
A critical component in determining surgical candidacy requires patient admission to the epilepsy monitoring unit for continuous scalp EEG and video monitoring. Correlation of the clinical seizure manifestations with interictal and ictal discharges helps localize the epileptogenic focus.
Provocative measures, such as medication reduction, sleep deprivation, and hyperventilation, may be used to help induce epileptiform activity. If scalp EEG fails to lateralize the epileptogenic focus, invasive EEG monitoring (an intracranial study) may be necessary to improve localization.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) has been well established as the best diagnostic modality for identifying lesions that are amendable to epilepsy surgery (lesional epilepsy).
Approximately 30% of patients undergoing epilepsy surgery have a structural epileptogenic lesion that can be localized with EEG recordings. Relatively new MRI techniques, such as fast fluid attenuation inversion recovery (FLAIR) imaging and high-resolution volumetric pulse sequences with spatial reconstruction, allow identification of small/subtle lesions that are amenable to surgery, such as neoplasms, arteriovenous/cavernous malformations, certain infections, gliosis, diffuse atrophic processes, migrational anomalies, hamartomas, and cortical dysplasias. Subtle foci of cortical dysplasias can be easily overlooked through conventional MRI techniques.
As many as 80%-90% of patients with frontal lobe epilepsy with a localizing structural lesion enjoy an excellent outcome after resection. Mosewich et al. found that 71% of patients with lesional FLE versus 41% with nonlesional FLE benefitted from excellent operative outcomes. This fact presents a major challenge because approximately 40%-50% of patients with FLE suffer from nonlesional epilepsy.
Positron Emission Tomography
Positron emission tomography (PET) utilizes radioactive isotopes linked to metabolically active molecules to analyze functionality in various regions of the body based on their metabolic activity.
When investigating FLE, PET seeks to localize regions of interictal hypometabolism in the frontal lobe. EEG recording during PET is important to ensure that hypometabolism in one hemisphere is not secondary to an active seizure focus on the contralateral side resulting in hypermetabolism.
Interictal PET has been shown to be more sensitive than MRI in detecting gliotic tissues with decreased fluorodeoxyglucose (FDG) uptake. However, gliotic tissue does not often localize to the epileptogenic focus. Less than half of the patients with hypometabolism found on PET demonstrate concordance with an abnormal EEG focus. PET hypometabolism in epilepsy is frequently widely distributed and poorly localizing. Overall, PET imaging has not been shown to provide additional clinically useful information when compared with MRI in patients with FLE.
Single Photon Emission Computed Tomography
Cerebral blood flow to the brain increases in regions of the brain undergoing seizure activity because of increased metabolic demand. Single photon emission computed tomography (SPECT) measures local cerebral perfusion using technetium-99m hexamethyl propylene amine oxime or technetium-99m bicisate.
These compounds are taken up by neurons within seconds of injection and remain within the cells for several hours. Therefore, the injection of radiotracers immediately following a seizure may help localize the seizure ictal onset area. The sensitivity of SPECT is increased if interictal studies are used to compare the relative change in cerebral perfusion during a seizure. Additionally, the difference in blood flow between interictal and ictal SPECT can be correlated to high-resolution MRI to identify the epilepsy focus. SPECT is typically reserved for cases in which MRI and/or EEG are nonlocalizing.
Invasive EEG Monitoring (Intracranial Study)
In many patients with frontal lobe epilepsy, scalp EEG, MRI, PET, and SPECT may not identify an epileptogenic focus or provide conflicting data on localization. In such cases, more invasive procedures, such as long-term EEG monitoring using epi/subdural or intraparenchymal strips and electrodes (intracranial study), should be used if there is a clear hypothesis about the localization of the focal epileptogenic zone. Please see the chapter on Intracranial Monitoring.
The seizure focus can usually be relatively lateralized to one hemisphere with noninvasive testing. The use of invasive monitoring must be used judiciously because it carries approximately a 1% risk of serious complications such as meningitis, bone flap necrosis, subdural hematoma, intraparenchymal hematoma, and herniation.
Subdural strips can be placed through a burr hole; this method is less invasive than the use of subdural grids, which require a craniotomy. The strips can provide an opportunity for focus lateralization before the grids are implanted. Grids are placed over most of the cortical surface and within the interhemispheric space, allowing a broad and comprehensive evaluation of the frontal cortex along with the opportunity for cortical mapping.
Functional Magnetic Resonance Imaging
Functional magnetic resonance imaging (fMRI) is used to examine neuronal activity by measurement of alterations of MRI signal caused by changes in blood oxygenation levels. Functional MRI is used mainly for localization of eloquent cortex, such as motor and language areas.
Additionally, it can be coupled with EEG analysis to identify the irritative zone and ictal onset zone. As a newer imaging modality, only a handful of studies have correlated fMRI and surgical outcome—all in the realm of temporal lobe epilepsy surgery. Further studies are necessary to elucidate the role of fMRI in frontal lobe surgery.
Indications for Surgery
Patients are considered for comprehensive epilepsy surgery evaluation if they suffer from seizures that are intractable despite: 1) correct seizure type and epilepsy syndrome diagnosis, 2) failure to achieve seizure control despite compliant use of at least two appropriate AEDs, and 3) absence of major medical comorbidities that contraindicate seizure surgery.
Seizure control must have a high probability of improving the patient’s quality of life. Certain seizure disorders are predictive of better outcomes. These disorders are associated with: 1) a well-circumscribed structural lesion as shown on MRI, 2) precise localization with EEG, 3) semiology features characteristic of frontal lobe epilepsy, 4) absence of discordance between clinical manifestations, EEG, and MRI findings, 5) a focus that is surgically accessible without involvement of eloquent cortex, and 6) absence of other epileptogenic foci (dural pathology).
Preoperative Considerations
The perioperative events and anesthetic medications lead to a drop in the serum levels of anticonvulsant medications, exposing the patient to the risks of postoperative seizures. Supratherapeutic levels of anticonvulsant medications are therefore advised during the perioperative period because seizures complicate the patient’s recovery from surgery.
I do not use intraoperative electrocorticography to guide the extent of neocortical or hippocampal resection. If the extent of seizure focus is in question, intracranial monitoring is more effective to guide the surgeon.
Operative Anatomy
The anatomy of the frontal lobe is relatively straightforward and familiar to most neurosurgeons.

Figure 1: The location of the coronal sutures in relation to the underlying frontal lobe is demonstrated. The parasagittal veins anterior to this suture are relatively dispensable. The extent of lobectomy should not reach posterior to the coronal suture as the motor cortex is about 3cm behind the suture (image courtesy of AL Rhoton, Jr).

Figure 2: The callosomarginal and pericallosal arteries are protected during the medial/interhemispheric transection of the lobe. The subpial resection technique protects these important arteries.
FRONTAL LOBECTOMY
Herein, the nuances of technique for a standard frontal lobectomy are described.

Figure 3: The above illustration outlines the oblique transection trajectory/line for the lobectomy. This line originates from the coronal suture and ends on the floor of the anterior cranial fossa. The dissection pathway stays anterior to the corpus callosum.

Figure 4: These sketches demonstrate the location of the posterior transection line for the lobectomy relative to the frontal horn and the sphenoid wing. The plane of transection (top) incorporates the coronal suture, and the lateral sphenoid wing. The plane ends anterior to the clinoid process. Note that the lateral border of the lobectomy is in line with the lateral sphenoid wing (bottom).

Figure 5: The patient's head is positioned in a skull clamp. The neck is slightly flexed to enhance cranial venous drainage. The ¾ bicoronal (Soutar) incision and the outlines of the bone flap are marked. The medial margin of the bone flap is on the superior sagittal sinus. This approach allows access to the interhemispheric fissure and the anterior cerebral arteries during resection of the frontal lobe. The posterior margin of the bone flap is the coronal suture. A single burr hole at the posterior edge of the bony exposure is adequate. Note that the anterior edge of the bone flap does not need to be parallel to the frontal fossa; the frontal sinus should not be entered.

Figure 6: The location of the single burr hole and the bony cuts for the craniotomy are illustrated. I typically complete the osteotomy over the dural venous sinus last. However, since compressive structural lesions are not present in this group of patients, the anterior superior sagittal sinus is readily dissected from the inner surface of the skull bone and is therefore unlikely to be injured by the footplate of the drill. The lateral edge of the craniotomy extends just beyond the superior temporal line. The temporalis muscle is only partially mobilized.
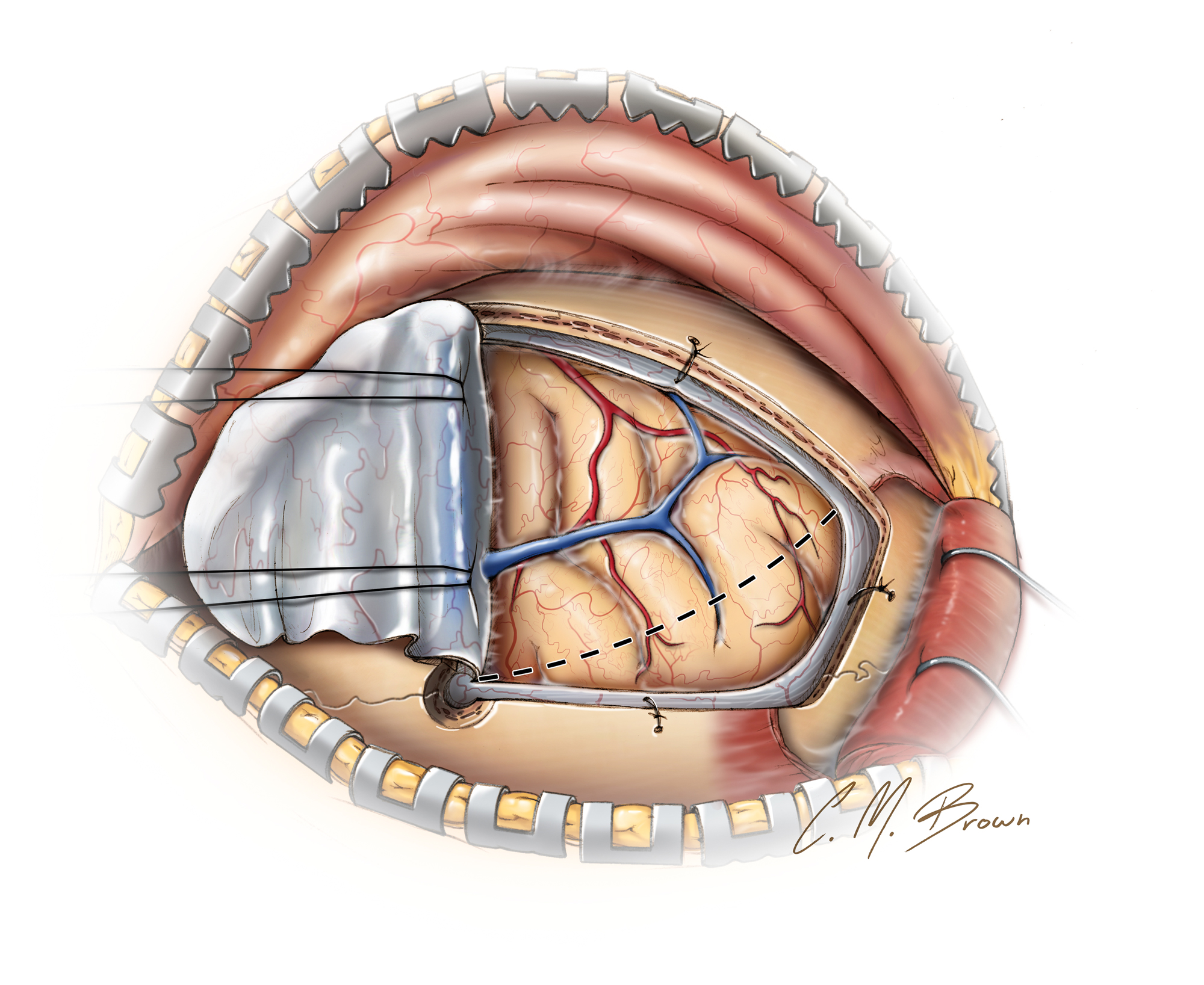
Figure 7: The dura is incised in a curvilinear pattern and reflected based on the dural sinus. Two retraction sutures are placed in the superior aspect of the falx; this maneuver gently mobilizes the dural sinus away from the interhemispheric dissection corridor. Note the outline of the superficial corticotomy (hashed lines). At this juncture, if the goal is only intracranial monitoring, the grids and strips are implanted and the incision closed.

Figure 8: The posterior corticotomy is extended into the white matter as illustrated. The bipolar forceps are used as scissors, disconnecting the white matter tracts. The anterior parasagittal draining veins are sacrificed.
Frontal lobectomy is carried out in two steps. First, the corticotomy of the lateral frontal lobe is performed, followed by a medial lobar transection around the corpus callosum and the anterior cingulate gyrus. The posterior orbital cortex is spared to avoid behavioral disturbances. Intraoperative image guidance may be utilized if desired.
I keep the above landmarks in mind during the entire dissection process. The oblique white matter dissection plane is extended toward the sphenoid wing. The anterior edge of the frontal horn may be avoided, if possible. The pial membranes along the medial frontal lobe are coagulated and cut. Just before reaching the cingulum, subpial resection continues so that the risk of injury to the anterior cerebral artery branches is minimized.

Figure 9: The subpial removal of the brain tissue is demonstrated. This important technique is frequently utilized in epilepsy surgery to protect the epipial en passage arteries. The pia is incised to the level of the cingulum (top) and the bipolar forceps are used to fragment the gyrus after which the suction device evacuates the fragmented tissue subpially. This maneuver completes the medial transection for the lobectomy.
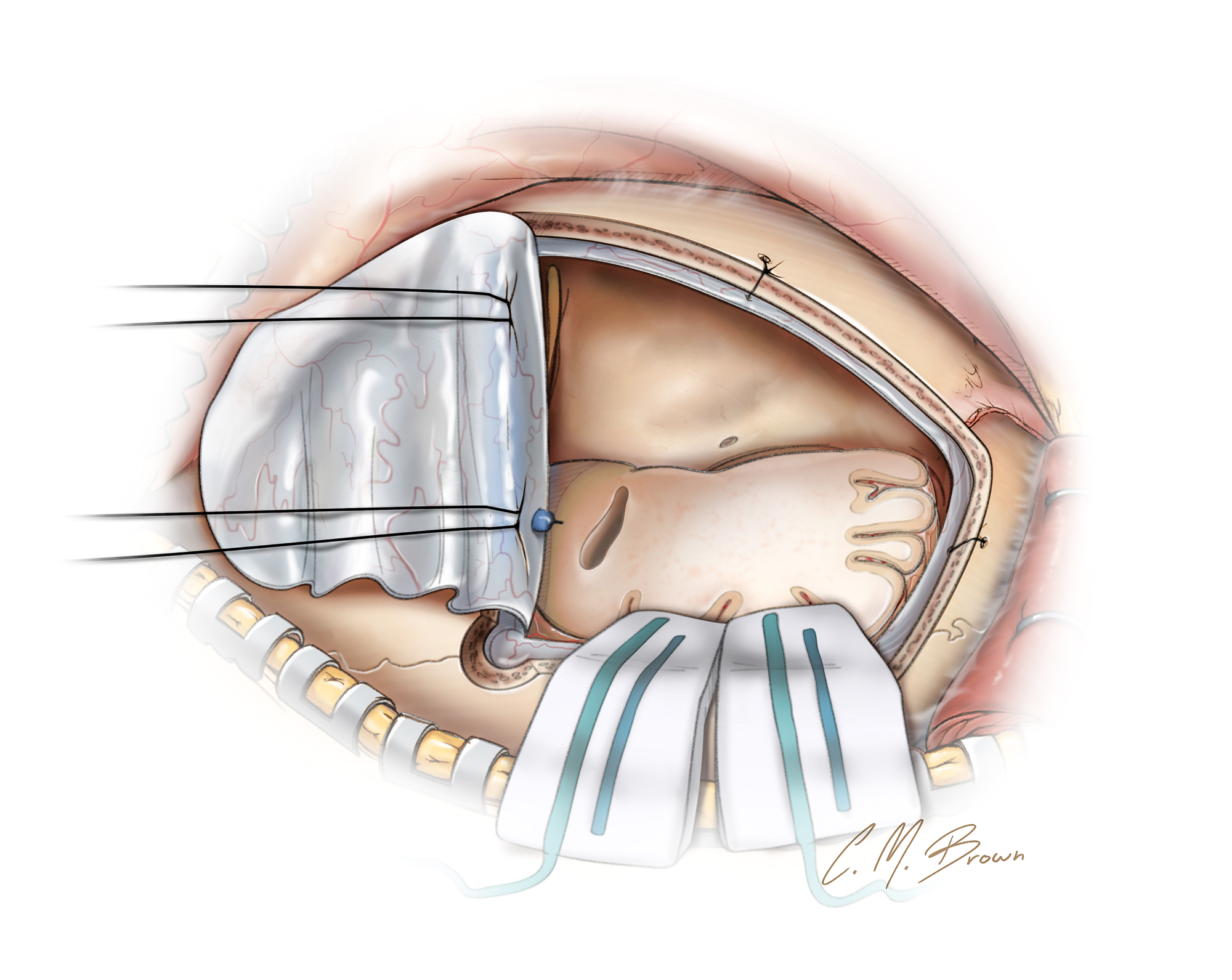
Figure 10: The result of resection is shown. If the frontal horn of the lateral ventricle is entered inadvertently, it is well irrigated.
Postoperative Considerations
The patient is observed in the intensive care unit overnight. Seizures during the immediate postoperative period do not affect the rate of long-term seizure freedom and the patient/family should be reassured in that regard. It may not be necessary to aggressively treat a single brief generalized seizure. If multiple seizures occur, the dosing of AEDs is adjusted appropriately.
AEDs are continued for 1-2 years after surgery, even if no seizures occur during this period.
Pearls and Pitfalls
- Coronal suture and the sphenoid wing are useful landmarks during frontal lobectomy.
- Subpial dissection avoids injury to the pericallosal and callosomarginal arteries.
Contributor: Stephen Mendenhall, MD
References
Bancaud J, Talairach J. Frontal lobe seizures and epilepsies, in Chauvel P, Delgado-Escueta AV, Halgren E, Bancaud J (eds): Advances in Neurology Frontal Lobe Seizures and Epilepsies, New York: Raven, 1992, 3-58.
Boon PA, Williamson PD, Fried I, et al. Intracranial, intraaxial, space-occupying lesions in patients with intractable partial seizures: an anatomoclinical, neuropsychological, and surgical correlation. Epilepsia. 1991;32:467-476.
Camfield PR, Camfield CS. Antiepileptic drug therapy: when is epilepsy truly intractable? Epilepsia. 1996;37 Suppl 1:S60-65.
Cockerell OC, Johnson AL, Sander JW, Hart YM, Shorvon SD. Remission of epilepsy: results from the National General Practice Study of Epilepsy. Lancet 1995;346:140-144.
Dasheiff RM, McNamara D, Dickinson L. Efficacy of second line antiepileptic drugs in the treatment of patients with medically refractive complex partial seizures. Epilepsia. 1986;27:124-127.
Engle J Jr, Shewmon DA. Overview: who should be considered a surgical candidate, in Engle J Jr (ed): Surgical Treatment of the Epilepsies, 2nd ed, New York: Raven, 1993, 23-34.
Heinz R, Ferris N, Lee EK, et al. MR and positron emission tomography in the diagnosis of surgically correctable temporal lobe epilepsy. AJNR Am J Neuroradiol. 1994;15:1341-1348.
Helmstaedter C, Kurthen M, Lux S, Reuber M, Elger CE. Chronic epilepsy and cognition: a longitudinal study in temporal lobe epilepsy. Ann Neurol. 2003;54:425-432.
Hermanns G, Noachtar S, Tuxhorn I, Holthausen H, Ebner A, Wolf P. Systematic testing of medical intractability for carbamazepine, phenytoin, and phenobarbital or primidone in monotherapy for patients considered for epilepsy surgery. Epilepsia. 1996;37:675-679.
Kwan P, Brodie MJ. Early identification of refractory epilepsy. N Engl J Med. 2000;342:314-319.
Ludwig B, Marsan CA, Van Buren J. Cerebral seizures of probable orbitofrontal origin. Epilepsia. 1975;16:141-158.
Ludwig BI, Marsan CA, Van Buren J. Depth and direct cortical recording in seizure disorders of extratemporal origin. Neurology. 1976;26:1085-1099.
Mirsattari SM, Ives JR, Leung LS, Menon RS. EEG monitoring during functional MRI in animal models. Epilepsia. 2007;48 Suppl 4:37-46.
Mohanraj R, Brodie MJ. Diagnosing refractory epilepsy: response to sequential treatment schedules. Eur J Neurol. 2006;13:277-282.
Mosewich RK, So EL, O'Brien TJ, et al. Factors predictive of the outcome of frontal lobe epilepsy surgery. Epilepsia. 2000;41:843-849.
Ojemann LM, Dodrill CB. Natural history of drug resistant seizures: clinical aspects. Epilepsy Res Suppl. 1992;5:13-17.
Proposal for revised classification of epilepsies and epileptic syndromes. Commission on Classification and Terminology of the International League Against Epilepsy. Epilepsia. 1989;30:389-399.
Quesney LF CM, Rasmussen T, Olivier A, Palmini A. Presurgical EEG investigation in frontal lobe epilepsy. Amsterdam: Elsevier, 1992.
Quesney LF, Olivier A. Pre-operative EEG evaluation in frontal lobe epilepsy. Acta Neurol Scand Suppl. 1988;117:61-72.
Schmidt D, Richter K. Alternative single anticonvulsant drug therapy for refractory epilepsy. Ann Neurol. 1986;19:85-87.
So EL. Integration of EEG, MRI, and SPECT in localizing the seizure focus for epilepsy surgery. Epilepsia. 2000;41 Suppl 3:S48-54.
Spanaki MV, Spencer SS, Corsi M, MacMullan J, Seibyl J, Zubal IG. Sensitivity and specificity of quantitative difference SPECT analysis in seizure localization. J Nucl Med. 1999;40:730-6.
Spencer SS. The relative contributions of MRI, SPECT, and PET imaging in epilepsy. Epilepsia. 1994;35 Suppl 6:S72-89.
Surgery for epilepsy: summary of a consensus statement. CMAJ. 1991;144:145-146.
Walczak TS, Leppik IE, D'Amelio M, et al. Incidence and risk factors in sudden unexpected death in epilepsy: a prospective cohort study. Neurology. 2001;56:519-525.
Westerhuis W, Zijlmans M, Fischer K, van Andel J, Leijten FS. Coping style and quality of life in patients with epilepsy: a cross-sectional study. J Neurol. 2011;258:37-43.
Wetjen NM, Cohen-Gadol AA, Maher CO, Marsh WR, Meyer FB, Cascino GD. Frontal lobe epilepsy: diagnosis and surgical treatment. Neurosurg Rev. 2002;25:119-138; discussion 139-140.
Wiebe S, Bellhouse DR, Fallahay C, Eliasziw M. Burden of epilepsy: the Ontario Health Survey. Can J Neurol Sci. 1999;26:263-270.
Wiebe S, Blume WT, Girvin JP, Eliasziw M, Effectiveness, Efficiency of Surgery for Temporal Lobe Epilepsy Study Group. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med. 2001;345:311-318.
Williamson PD, Spencer DD, Spencer SS, Novelly RA, Mattson RH. Complex partial status epilepticus: a depth-electrode study. Ann Neurol. 1985;18:647-654.
Related Materials
Available Through the Atlas
-

Importance of veins in partial cerebral lobectomy
-
Surgical outcome and prognostic factors of frontal lobe epilepsy...
Unavailable Through the Atlas
Please login to post a comment.




