

Trochlear Nerve

ABSTRACT
The trochlear nerve is the cranial nerve with the longest intracranial course, but also the thinnest. It is the only nerve that arises from the dorsal surface of the brainstem and decussates in the superior medullary velum. After leaving the dorsal surface of the brainstem, it courses anterolaterally around the lateral surface of the brainstem and then passes anteriorly just beneath the free edge of the tentorium. It passes forward to enter the cavernous sinus, traverses the superior orbital fissure and terminates in the superior oblique muscle in the orbit. Because of its small diameter and its long course, the trochlear nerve can easily be injured during surgical procedures. Therefore, precise knowledge of its surgical anatomy and its neurovascular relationships is essential for approaching and removing complex lesions of the orbit and the middle and posterior fossae safely. This review describes the microsurgical anatomy of the trochlear nerve and is illustrated with pictures involving the nerve and its surrounding connective and neurovascular structures.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
INTRODUCTION
The trochlear nerve is the cranial nerve with the longest intracranial course (60 mm) but also the smallest diameter (0.75–1.0 mm) (Villain et al., 1993). It is a pure general somatic efferent nerve that innervates the superior oblique muscle, which depresses, intorts, and abducts the eye. It is divided into brainstem, cisternal, tentorial, cavernous, and orbital segments (Ammirati et al., 2002; Bisaria, 1988; Zhang et al., 2010; Gupta et al., 2014).
BRAINSTEM SEGMENT
The trochlear nucleus is one of the smallest motor nuclei in the brainstem, though the precise morphology has not been fully investigated in humans (Yamaguchi and Honma, 2011). This nucleus is in the ventral grey matter near the midline at the level of the inferior colliculus. With the medial longitudinal fasciculus running immediately ventral to it, the nucleus extends through the lower half of the midbrain, just caudal to the oculomotor nucleus. It is located at the caudal end of the oculomotor nucleus and between the dorsum of the red nucleus and the ventrolateral area of periaqueductal gray matter in the midbrain on surface models (Park et al., 2015). Trochlear efferent fibers pass posterolaterally round the central grey matter, then descend medial to the trigeminal mesencephalic nucleus to reach the upper end of the superior medullary velum, where they decussate and merge lateral to the frenulum of the superior medullary velum under the inferior colliculi (Gray et al., 1989).
CISTERNAL SEGMENT
The trochlear nerve emerges from the dorsal midbrain as a single root, immediately lateral to the lower edge of the inferior colliculus (Figs. 1A and 1B) (Ammirati et al., 2002). However, some literature reports that it originates 461 mm lateral to the midline through a variable number (one to four) of rootlets (Villain et al., 1993; Iaconetta et al., 2013). The initial part of the cisternal segment of the trochlear nerve is followed laterally in the cerebellomesencephalic fissure. The nerve crosses to the lateral side of the superior cerebellar peduncle and winds round the cerebral peduncle just above the pons toward the tentorium through the quadrigeminal and ambient cisterns (Figs. 1C and 1D). In its initial cisternal segment, the trochlear nerve is readily visible in the subarachnoid space, but once it reaches the free edge of the tentorium and passes along its inferior surface it becomes difficult to identify from the surgeon’s direct view (Figs. 1D, and 2A). Therefore, incision of the tentorium has to be planned so as to minimize the chances of trochlear nerve injury (Fig. 2D). The maximum length of tentorium covering the cisternal segment ranges from 0.5 to 6 mm with a mean of 2 mm (Tubbs and Oakes, 1998).
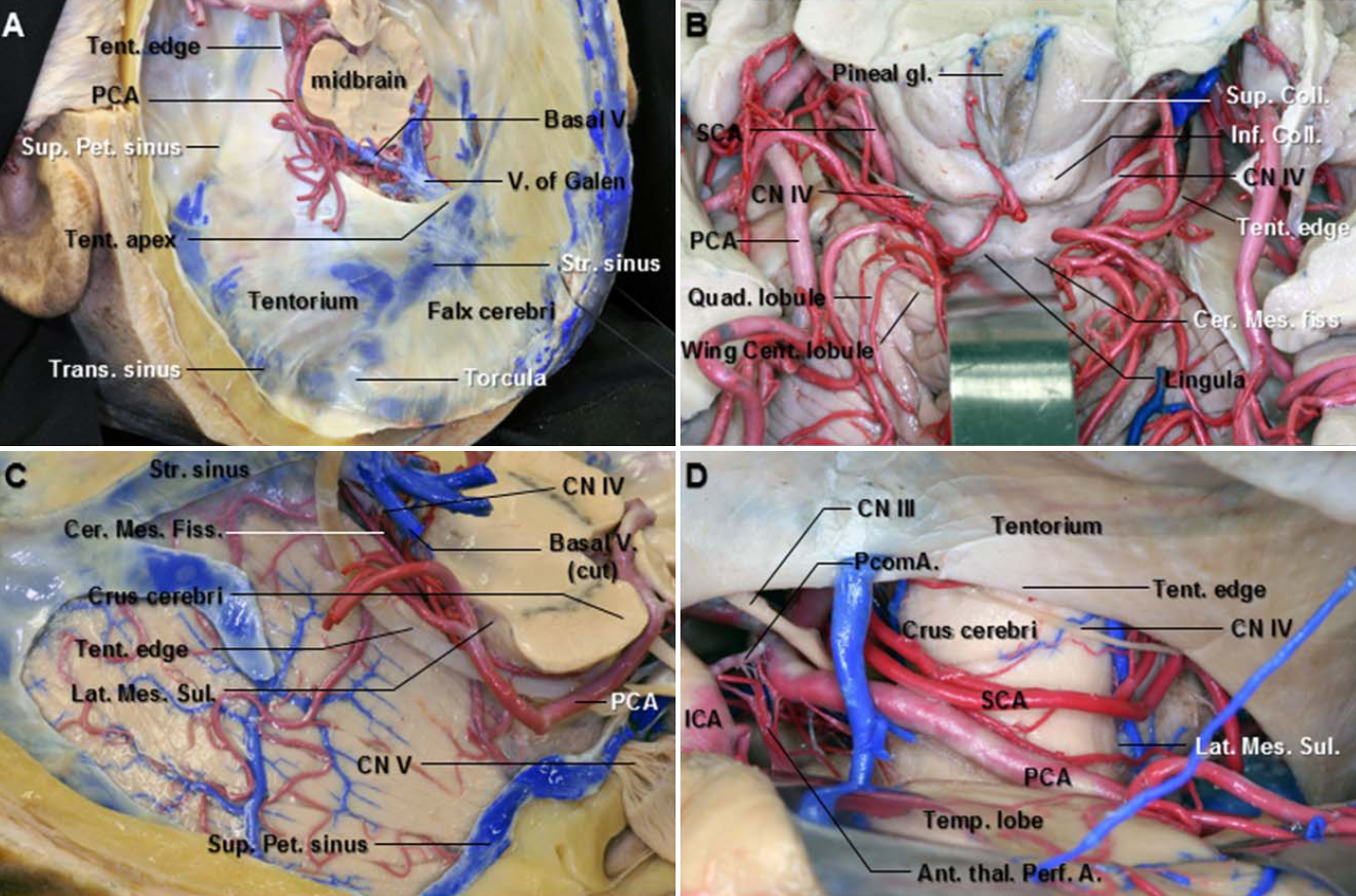
Figure 1. A. Superolateral view of the falx and tentorium after removing the cerebrum. The tentorial edges sweep along the lateral margin of the cerebral peduncle. The tentorial apex is located at the junction of the vein of Galen and the straight sinus. The tentorial edges slope downward from the apex. B. Superoposterior view of the cerebellomesencephalic fissure. The central lobule and culmen of the cerebellar vermis have been retracted posteriorly to expose the cerebellomesencephalic fissure, which extends forward between the cerebellum and midbrain. The anterior wall of the fissure is formed in the midline by the collicular plate and lingual, and laterally by the superior cerebellar peduncles. The trochlear nerve arises below the inferior colliculi. The initial part of the cisternal segment of the trochlear nerve is followed laterally in the cerebellomesencephalic fissure. C. Superolateral view of the right tentorial surface of the cerebellum. The tentorial edge sweeps along the lateral margin of the cerebral peduncle. The tentorium has been removed while the tentorial venous sinuses and tentorial edge have been preserved. The posterior cerebral artery runs posteriorly along the lateral margin of the midbrain above the tentorial edge. D. Subtemporal view. The right temporal lobe has been elevated to expose the PCA, SCA, and trochlear nerve in the anterior and middle incisural spaces. The PCA passes above and the SCA below the oculomotor nerve. The trochlear nerve courses around the side of the brainstem. It becomes subtentorial at the anterolateral part of the cerebral peduncle. Ant. Thal. Perf. A., anterior thalamoperforating artery; Cent., central; Cer. Mes. Fiss., cerebellomesencephalic fissure; CN., cranial nerve; Coll., colliculus; ICA., internal carotid artery; Inf., inferior; Lat. Mes. Sul., lateral mesencephalic sulcus; PCA., posterior cerebral artery; PcomA., posterior communicating artery; Pet., petrosal; Quad., quadrangular; SCA., superior cerebellar artery; Str., straight; Sup., superior; Tent., tentorium; Temp., temporal; Trans., transverse; V., vein. (Images courtesy of AL Rhoton, Jr.)

Figure 2. A. Superior view. The uncus has been retracted laterally to expose the tentorial edge and the trochlear nerve. The trochlear nerve runs anteriorly along the tentorial edge to pierce the dura at the level of the rostrolateral free edge of the tentorium posterior to the posterolateral margin of the oculomotor triangle. Two margins of the oculomotor triangle are formed by the anterior and posterior petroclinoidal dural folds that extend, respectively, from the anterior and posterior clinoid processes to the petrous apex. B. The tentorial edge has been retracted laterally to expose the trochlear nerve and its groove on the tentorium. The trochlear nerve entrenches itself progressively in a groove on the lower surface of the free tentorial edge. The groove is a smooth transition from the free cisternal segment to the definitive fixed dural entry point. C. Enlarged view of B. The dura overlying the oculomotor and trochlear nerves has been incised and retracted laterally to expose the oculomotor and trochlear cisterns. The oculomotor nerve has an impression at the dural penetration site. D. The right combined presigmoid approach to expose the upper cerebellopontine angle and petrous apex. The presigmoid dura is opened from the anterior jugular bulb toward the superior petrosal sinus with a cut made superior to the transverse sinus toward the superior petrosal sinus, which can then be ligated and cut. The tentorium is cut posterior to the superior petrosal sinus toward the tentorial edge, taking care to avoid the trochlear nerve. Retractors are then placed using the tentorium between the retractor blade and the temporal lobe to protect the underlying temporal lobe cortex. The trochlear nerve courses under the tentorium behind the superior petrosal sinus. A., artery; Ant., anterior; Bas., basilar; CN., cranial nerve; Interped., interpeduncular; Jug., jugular; Oculom., oculomotor; Parahippo., parahippocampal; penet., penetration; Petroclin., petroclinoid; PCA., posterior cerebral artery; PcomA., posterior communicating artery; PCP., posterior clinoid process; Pet., petrosal; SCA., superior cerebellar artery; Semi., semicircular; Sig., sigmoid; Sup., superior; V., vein. (Images courtesy of AL Rhoton, Jr.)
Iaconetta et al. divided the cisternal segment into quadrigeminal and ambient divisions according to their location, relationships, and clinical and surgical considerations (Iaconetta et al., 2013). The quadrigeminal segment curves along an anterolateral and slightly inferior trajectory toward the lateral aspect of the cerebral peduncle in the pontomesencephalic fissure and remains free within the subarachnoid space as far as the ambient cistern mesh (Fig. 1B). The trochlear nerve pierces the cerebellar precentral membrane that forms the lateral wall of the quadrigeminal cistern to enter the ambient cistern (Lu and Zhu, 2007; Iaconetta et al., 2013). The ambient segment of the trochlear nerve has relationships with the superior cerebellar artery, posterior cerebral artery, basal vein of Rosenthal, and the lateral aspect of the midbrain (Figs. 1C and 1D). All trochlear nerves studied by Herlan et al. (2013) were entrenched progressively in a groove on the lower surface of the free tentorial edge. Because the groove is a smooth transition from the free cisternal segment to the definitive fixed dural entry point, it is not feasible to measure its effective length accurately (Figs. 2B and 2C) (Herlan et al., 2013). We suggest that the part of the trochlear nerve passing along the infratentorial groove of the tentorium might be included in the tentorial segment, as reviewed below. The distal limit of the cisternal segment of the trochlear nerve is represented by the point where the nerve begin to run in the groove on the inferior surface of the tentorium before being completely encased in the dural canal (Fig. 2C). Consequently, the cisternal segment, including the nerve underneath the tentorium, not in the groove, is relatively free and therefore more likely to be stretched or distorted by pathologies along its course (Figs. 2A and 2B). However, Tubbs and Oakes defined the cisternal segment as extending from the origin of the trochlear nerve on the dorsal brain stem to its dural entrance. Given this definition, the length of the cisternal segment ranged from 24 to 45 mm (mean 35.6 mm) (Tubbs and Oakes, 1998).
From the surgical point of view, the cisternal segment can easily be exposed without dural dissection. The quadrigeminal and ambient divisions are observed with different approaches (Ammirati et al., 2002; Iaconetta et al., 2013). The quadrigeminal division can be accessed through different posterior fossa approaches, such as the mid-line or paramedian infratentorial-supracerebellar approach, while the ambient division can be accessed through the lateral transtentorial approach. The extreme lateral infratentorial-supracerebellar approach clearly exposes the junction between the quadrigeminal and ambient segments of the nerve. Using this approach, the trochlear nerve is usually immediately evident in the ambient cistern but when it runs close to the free tentorial margin it is not easily recognized. In such cases the cerebellomesencephalic segment of the superior cerebellar artery is a good landmark to identify; it is usually located above it, all along the posterior and lateral aspects of the midbrain (Figs. 1C, 1D, and 2D). The combined presigmoid subtemporal transtentorial approach is suitable for exposing the junction between the cisternal and tentorial segments (Fig. 2D) (Ammirati et al., 2002).
TENTORIAL SEGMENT
The trochlear nerve pierces the dura at the level of the rostrolateral free edge of the tentorium cerebelli posterior to the posterolateral margin of the oculomotor triangle (Figs. 2A–2C). Traditionally, it has been termed the cavernous segment when it pierces the free edge of the tentorium (Bisaria, 1988; Ammirati et al., 2002; Mercier et al., 2009). The tentorial segment extends from the entrance of the trochlear nerve into the tentorium to the anterior petroclinoid fold where the nerve enters the cavernous sinus. The length and width of the tentorial segment are 9.3161.49 and 0.960.4 mm, respectively (Iaconetta et al., 2013).
Rhoton et al. noted that the trochlear nerve courses a short distance in the posterior petroclinoid fold just after piercing the tentorium, which is the trochlear cistern. Within the cistern, the trochlear nerve does not become incorporated into the lateral wall of the cavernous sinus until it reaches the tip of the anterior clinoid process (Fig. 2C) (Rhoton, 2000). Tubbs et al. described this portion of the tentorial segment, which was enveloped by an arachnoid fold, and termed it a trigonal segment. Its length ranges from 2.2 to 6 mm with a mean of 4 mm (Tubbs et al., 2014). Compared to the cisternal segment, which is relatively free, the fixed tentorial segment includes the nerve passing along the groove under the tentorium and trigonal segments, as named by Tubbs et al. Therefore, we consider the trigonal segment as the distal part of the tentorial segment of the trochlear nerve.
From a neurosurgical standpoint, retraction of the trochlear nerve outside the cavernous sinus can be facilitated by opening the dura covering the trigonal segment because no venous or arterial structures are accompanied by this segment. The presence of a cistern around the nerve, rather than the nerve being tightly bound in the dura, adds a margin of safety to the exposure of the nerve in the roof of the sinus (Fig. 2C). However, Ammirati et al. reported a tight relationship between the nerve and the tentorial dura in its tentorial segment, making dissection very difficult despite the presence of the arachnoid sleeve (Ammirati et al., 2002).
Localizing the tentorial segment of the trochlear nerve in the lateral incisural space can be difficult, particularly from the supratentorial approach. Furthermore, tumors can displace it from its normal anatomical course. In general, the trochlear nerve first becomes subtentorial or abuts the tentorium at the posterior border of the cerebral peduncle (Figs. 1D and 2D). This is the point at which the surgeon can first lose sight it from the supratentorial approach. It is generally 1.5–2 cm posterior to the most external portion of the external auditory meatus (EAM). It is interesting to remember that the external auditory meatus lies on the same coronal plane as the internal auditory meatus (Figs. 3D and 4A). Therefore, an imaginary line drawn from the external to the internal acoustic canal can be used as a reference line. If one then stays at least 1.5 cm behind this line and incises the tentorium at that distance posterior to it, one can avoid injury to the trochlear nerve (Tubbs and Oakes, 1998). The tentorial segment of the trochlear nerve comes into view after the tentorium has been sectioned.

Figure 3. A. The outer layer of the dura of the right cavernous sinus has been peeled away from the lateral wall of the cavernous sinus and Meckel’s cave. This exposes the oculomotor and trochlear nerves entering the roof of the cavernous sinus and passing forward through the superior orbital fissure. The superior petrosal sinus passes above the ostium of Meckel’s cave and joins the posterior part of the cavernous sinus. B. The remaining dura covering the lateral wall of the cavernous sinus has been removed. The trochlear nerve courses along the inferior aspect of the oculomotor nerve to the base of the anterior clinoid process. C. After the anterior clinoid process has been removed, the clinoid segment of the internal carotid artery is exposed. The oculomotor nerve enters a short cistern in the sinus roof and does not become incorporated into the lateral wall until it reaches the lower margin of the anterior clinoid process. The tentorial artery courses along the inferior surface of the trochlear nerve and runs with it to the superior orbital fissure. D. Overview. The posterior wall of the cavernous sinus extends laterally from the dorsum sellae to the medial edge of the ostium of Meckel’s cave. The floor of the middle fossa has been removed to expose the infratemporal fossa, which contains the branches of the maxillary artery and the mandibular nerve, the pterygoid venous plexus, and the pterygoid muscle. The trochlear nerve courses around the cerebral peduncle just above the pons, between the posterior cerebral and superior cerebellar arteries. It pierces the dura below the free edge of the tentorium cerebelli, just behind the posterior clinoid process, and then passes forward in the lateral wall of the cavernous sinus below the oculomotor nerve and above the ophthalmic division of the trigeminal nerve. The trochlear nerve crosses the oculomotor nerve at the level of the optic strut, entering the orbit by the superior orbital fissure above the annular tendon and medial to the frontal nerve. A., artery; ACA., anterior clinoid process; Clin., clinoid; CN., cranial nerve; For., foramen; GSPN., great superficial petrosal nerve; IAM., internal acoustic meatus; ICA., internal carotid artery; Lat., lateral; M., muscle; PCA., posterior cerebral artery; PCP., posterior clinoid process; Pteryg., pterygoid; SOF., superior orbital fissure; Tent., tentorial. (Images courtesy of AL Rhoton, Jr.)

Figure 4. A. The lesser wing of the sphenoid bone forming the roof of the superior orbital fissure has been removed to expose the contents of the fissure. The trochlear nerve and the frontal nerve, a branch of the ophthalmic division of the trigeminal nerve, enter the orbit through superior orbital fissure above the annular tendon. B. The orbital roof of the right orbit has been removed to expose the periorbita. At the superior orbital fissure, dura covering the middle fossa and cavernous sinus blends into the periorbita of the orbital apex and into the annular tendon from which the rectus muscle arises. The dura lining the superior orbital fissure and optic sheath blends into the periorbita. C. The periorbita has been opened and retracted laterally to expose the orbital fat, in which the trochlear, frontal, and lacrimal nerves course. D. The orbital fat has been removed. The ophthalmic nerve divides into the lacrimal, frontal, and nasociliary nerves. The trochlear nerve passes medially above the levator muscle to reach the superior oblique muscle. The tendon of the superior oblique muscle passes through the trochlea and below the superior rectus muscle to insert on the globe between the attachment of the superior rectus and lateral rectus muscles. The lacrimal nerve passes above the lateral rectus muscle to innervate the lacrimal gland. E. Enlarged view of the superior orbital fissure from above. The dura lining the right superior orbital fissure has been removed to expose the course of the trochlear nerve from the cavernous sinus to the orbit. ACP., anterior clinoid process; CN., cranial nerve; Falc., falciform; Gl, gland; IAM., internal acoustic meatus; Lac., lacrimal; Lat., lateral; Lev., levator; Lig., ligament; M., muscle; N., nerve; Nasocil, nasociliary; Obl., oblique; PCA., posterior cerebral artery; Pit., pituitary; Rec., rectus; SCA., superior cerebellar artery; SOF., superior orbital fissure; Sph., sphenoid; Sup., superior. (Images courtesy of AL Rhoton, Jr.)
CAVERNOUS SEGMENT
The cavernous segment extends from the point at which the trochlear nerve inserts into the lateral wall of the cavernous sinus to the superior orbital fissure. The trochlear nerve enters the roof of the cavernous sinus in the posterolateral apex of the oculomotor triangle, 8.1262.32 mm (range, 4.52–13.1 mm) behind the entrance of the oculomotor nerve and 13.8262.39 mm (range, 10.14–20.1 mm) posterolateral to the posterior clinoid process (Figs. 2A and 2B) (Yasuda et al., 2005). In 77.5% of cases (62 out of 80 cavernous sinuses) it showed a marked bend and flattening at the site of its penetration into the dura (Bisaria, 1988). After penetrating the roof of the cavernous sinus at the junction of the anterior and posterior petroclinoid dural folds, the cavernous segment of the trochlear nerve after the trigonal segment, the distal part of the tentorial segment, courses in the lateral wall of the cavernous sinus below the oculomotor nerve. The proximal part of the cavernous segment passes between the oculomotor nerve superiorly and ophthalmic nerve inferiorly (Fig. 3). The distance between the oculomotor and trochlear nerves is 1 mm, while the distance between the trochlear and ophthalmic nerves is 2.5 mm (Iaconetta et al., 2013). In 72.5% of cases (58 out of 80 cavernous sinuses), the diameter of the trochlear nerve increased during its passage from its entrance into the cavernous sinus to its exit through the superior orbital fissure, and in 20% of cases such an increase in thickness was noted even in the posterior cranial fossa (Bisaria, 1988) (Figs. 3C and 3D). The length and width of the cavernous segment of the trochlear nerve were 20.3861.95 and 0.960.4 mm, respectively (Iaconetta et al., 2013). At the level of the optic strut, the trochlear nerve crosses, laterally to medially, between the upper surface of the oculomotor nerve and the dura lining the lower margin of the anterior clinoid process and optic strut, and becomes the most superior structure of the cavernous sinus (Figs. 3D and 4A).
The trochlear nerve also forms the upper margin of Parkinson’s triangle in the lateral wall of the cavernous sinus. This triangle is situated between the lower margin of the trochlear nerve and the upper margin of the ophthalmic nerve. The third margin is formed by a line connecting the point of entry of the trochlear nerve into the dura to the site where the trigeminal nerve enters Meckel’s cave. The posterior bend of the internal carotid artery and the origin of the meningohypophyseal trunk from the posterior bend are located in this triangle, except when the carotid artery is elongated and tortuous (Fig. 3D).
The proximal part of the trochlear nerve in the cavernous sinus is constantly supplied by the superoproximal artery, a branch of the inferolateral trunk. This artery follows the superior surface of the trochlear nerve along the lateral wall of the cavernous sinus. This constant relationship can be used during transcranial microsurgical surgery to help identify the nerve by the presence of the artery (Lang and Kageyama, 1990; Krisht et al., 1994; d’Avella et al., 2008). It has been demonstrated that the distal part of the nerve is supplied in most cases by the tentorial artery through the endoscopic trans-sphenoidal route. The tentorial artery reaches the nerve on its inferior surface and runs with it to the superior orbital fissure (Fig. 3C) (d’Avella et al., 2008).
ORBITAL SEGMENT
The trochlear nerve crosses the upper surface of the oculomotor nerve, laterally to medially, and enters the orbit through the superior orbital fissure as the most superior of all nerves entering the orbit (Figs. 4A, 4D, and 4E). The superior orbital fissure is a small but topographically important area that connects the middle cranial fossa and orbit. It is divided into the superolateral and inferomedial parts (Figs. 4A and 4E) (Morard et al., 1994; Natori and Rhoton, 1995; Govsa et al., 1999). The trochlear nerve is the structure closest to the superior rim of the superior orbital fissure. The superior or superolateral part includes the trochlear, lacrimal, and frontal nerves and the superior ophthalmic vein. The inferior or inferomedial part includes the superior and inferior branches of the oculomotor, nasociliary, and abducens nerves and the sympathetic root to the ciliary ganglion (Govsa et al., 1999; Reymond et al., 2008). The orbital segment of the trochlear nerve emerges in the lateral region of the superior orbital fissure, just lateral to the lateral edge of the annulus of Zinn, passing superomedially to the frontal nerve (Figs. 4D and 4E). The trochlear, frontal, and lacrimal nerves course in the orbital fat just beneath the periorbita (Figs. 4B and 4C).
The trochlear nerve is located on the lateral side of the optic nerve near the orbital apex that passes above the optic nerve to reach the superior oblique muscle. From a surgical point of view, the incision for opening the annular tendon, if needed, should be directed between the attachments of the superior and medial rectus muscles. Before the annulus is opened, the trochlear nerve should be separated from the adjacent tissue above the orbital apex to prevent injury to it when the optic sheath is opened (Fig. 4E) (Natori and Rhoton, 1994; Rhoton, 2002; Zhang et al., 2010). After passing the superior orbital fissure, the nerve travels medially and diagonally across the levator palpebrae superior and superior rectus muscles to reach the superior oblique muscle.
The superior oblique muscle arises from the periorbita covering the body of the sphenoid bone superomedial to the optic canal and runs forward, ending in a tendon that loops through the trochlea, a round tendon that attaches to the trochlear fossa of the frontal bone. After looping through the trochlea, the tendon passes laterally and posteriorly below the superior rectus muscle to insert on the sclera between the superior and lateral rectus muscles. The nerve gives off an average of six branches (range 4–10) (Fig. 4D). The branches of the trochlear nerve end on the posterior one-third of the superior oblique muscle in 76% of cases (76 out of 100 orbits) and on the middle one-third in 24%. Penetration of the trochlear nerve into the muscle starts 17.25 mm from the origin of the muscle and extends for 7 mm (the average length of the superior oblique muscle is 40.6 mm) (Villain et al., 1993; Zhang et al., 2010). The trochlear nerve terminates at the superior oblique muscle on the medial aspect in 23 cases out of 30 (77%), on the superior edge in seven (23%), but never on the lateral aspect; the mean length of the orbital segment of the nerve is 25.1 mm (range 18–34 mm) (Villain et al., 1993). The vascular supply to the orbital segment of the trochlear nerve is provided by the terminal branches of both the ophthalmic and the anterior meningeal arteries (Iaconetta et al., 2013).
CONCLUSIONS
The trochlear nerve is the smallest of the cranial nerves and yet it has the longest intracranial course. It is the only cranial nerve arising from the dorsal aspect of the brain stem and the only one of which the fibers decussate. Because the trochlear nerve courses through supracerebellar, incisural, cavernous sinus, and orbital areas, accurate knowledge of its anatomy and that of its surrounding structures is important for avoiding injury to it during surgical procedures.
Contributors: Wonil Joo and Albert L. Rhoton, Jr
Content from Joo W, Rhoton AL, Jr. Microsurgical anatomy of the trochlear nerve. Clin Anat 2015;28:857–864. doi.org/10.1002/ca.22602.
The Neurosurgical Atlas is honored to maintain the legacy of Albert L. Rhoton, Jr, MD.
References
- Ammirati M, Musumeci A, Bernardo A, Bricolo A. 2002. The microsurgical anatomy of the cisternal segment of the trochlear nerve, as seen through different neurosurgical operative windows. Acta Neurochir 144:1323–1327.
- Bisaria KK. 1988. Cavernous portion of the trochlear nerve with special reference to its site of entrance. J Anat 159:29–35.
- d’Avella E, Tschabitscher M, Santoro A, Delfini R. 2008. Blood supply to the intracavernous cranial nerves: comparison of the endoscopic and microsurgical perspectives. Neurosurgery 62:ONS305-310; discussion ONS310-301.
- Govsa F, Kayalioglu G, Erturk M, Ozgur T. 1999. The superior orbital fissure and its contents. Surg Radiol Anat 21:181–185.
- Gray H, Williams PL, Gray H. 1989. The mesencepahlon ormidbrain. In: Gray’s Anatomy. 37th Ed. Edinburgh; New York: C. Livingstone.
- Gupta T, Gupta SK, Sahni D. 2014. Anatomy of the tentorial segment of the trochlear nerve in reference to its preservation during surgery for skull base lesions. Surg Radiol Anat 36:967–971.
- Herlan S, Hirt B, Tatagiba M, Ebner FH. 2013. Focus on the Lateral Incisural Space: Where is the Trochlear Nerve?. J Neurol Surg B Skull Base 74:271–273.
- Iaconetta G, de Notaris M, Benet A, Rincon J, Cavallo LM, Prats-Galino A, Samii M, Cappabianca P. 2013. The trochlear nerve: Microanatomic and endoscopic study. Neurosurg Rev 36:227–237. discussion 237-228.
- Krisht A, Barnett DW, Barrow DL, Bonner G. 1994. The blood supply of the intracavernous cranial nerves: An anatomic study. Neurosurgery 34:275–279. discussion 279.
- Lang J, Kageyama I. 1990. Clinical anatomy of the blood spaces and blood vessels surrounding the siphon of the internal carotid artery. Acta Anat (Basel) 139:320–325.
- Lu J, Zhu XL. 2007. Cranial arachnoid membranes: some aspects of microsurgical anatomy. Clin Anat 20:502–511.
- Mercier P, Brassier G, Fournier HD, Delion M, Papon X, Lasjaunias P. 2009. [Morphological anatomy of the cranial nerves in their cisternal segment (III-XII)]. Neuro Chirurgie 55:78–86.
- Morard M, Tcherekayev V, de Tribolet N. 1994. The superior orbital fissure: a microanatomical study. Neurosurgery 35:1087–1093.
- Natori Y, Rhoton AL. Jr. 1994. Transcranial approach to the orbit: microsurgical anatomy. Journal of Neurosurgery 81:78–86.
- Natori Y, Rhoton AL. Jr. 1995. Microsurgical anatomy of the superior orbital fissure. Neurosurgery 36:762–775.
- Park HS, Chung MS, Shin DS, Jung YW, Park JS. 2015. Whole courses of the oculomotor, trochlear, and abducens nerves, identified in sectioned images and surface models. Anat Record 298:436–443.
- Reymond J, Kwiatkowski J, Wysocki J. 2008. Clinical anatomy of the superior orbital fissure and the orbital apex. J Craniomaxillofac Surg 36:346–353.
- Rhoton AL. Jr. 2000. Tentorial incisura. Neurosurgery 47:S131–S153.
- Rhoton AL. Jr. 2002. The orbit. Neurosurgery 51:S303–S334.
- Tubbs RS, Oakes WJ. 1998. Relationships of the cisternal segment of the trochlear nerve. J Neurosurg 89:1015–1019.
- Tubbs RS, Veith P, Griessenauer CJ, Loukas M, Cohen-Gadol AA. 2014. A new segment of the trochlear nerve: cadaveric study with application to skull base surgery. J Neurol Surg B Skull Base 75:8–10.
- Villain M, Segnarbieux F, Bonnel F, Aubry I, Arnaud B. 1993. The trochlear nerve: anatomy by microdissection. Surg Radiol Anat 15:169–173.
- Yamaguchi K, Honma K. 2011. Development of the human trochlear nucleus: a morphometric study. Annals of Anatomy: Official Organ of the Anatomische Gesellschaft 193:106–111.
- Yasuda A, Campero A, Martins C, Rhoton AL, Jr., de Oliveira E, Ribas GC. 2005. Microsurgical anatomy and approaches to the cavernous sinus. Neurosurgery 56:4–27. discussion 24-27.
- Zhang Y, Liu H, Liu EZ, Lin YZ, Zhao SG, Jing GH. 2010. Microsurgical anatomy of the ocular motor nerves. Surg Radiol Anat: SRA 32:623–628.
Please login to post a comment.




