

Anterior Clinoidectomy and Optic Nerve Decompression

ABSTRACT
BACKGROUND: Several diseases that involve the optic canal or its contained structures may cause visual impairment. Several techniques have been developed to decompress the optic nerve.
OBJECTIVE: To describe minimally invasive extradural anterior clinoidectomy (MiniEx) for optic nerve decompression, detail its surgical anatomy, present clinical cases, and established a proof of concept.
METHODS: Anatomic dissections were performed in cadaver heads to show the surgical anatomy and to show stepwise the MiniEx approach. In addition, these surgical concepts were applied to decompress the optic nerve in 6 clinical cases.
RESULTS: The MiniEx approach allowed the extradural anterior clinoidectomy and a nearly 270° optic nerve decompression using the no-drill technique. In the MiniEx approach, the skin incision, dissection of the temporal muscle, and craniotomy were smaller and provided the same extent of exposure of the optic nerve, anterior clinoid process, and superior orbital fissure as that usually provided by standard techniques. All patients who underwent operation with this technique had improved visual status.
CONCLUSIONS: The MiniEx approach is an excellent alternative to traditional approaches for extradural anterior clinoidectomy and optic nerve decompression. It may be used as a part of more complex surgery or as a single surgical procedure.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
INTRODUCTION
Several diseases that involve the optic canal or its contents may cause orbitopathy, with consequent visual impairment.1,2 Fronto-orbital trauma (caused either by a fracture of the optic canal or by intraneural contusion, vasospasm, necrosis, or edema), intracranial tumors (meningiomas of the tuberculum sellae or of the sphenoid bone and optic nerve gliomas), secondary lesions (mucocele, paranasal orbit-sinusal neoplasms), fibrous or bony dysplasia, inflammatory pseudotumors, Graves orbitopathy, or vascular lesions (carotid-ophthalmic aneurysms) are the most common diseases that may compress the optic nerve.3–5 Numerous reports have shown that early decompression of the canalicular segment of the optic nerve improves visual outcomes.5–13
Minimally invasive craniotomies have increasingly become a popular alternative for traditional craniotomies in many surgical scenarios (e.g., vascular and skull base procedures). Compared with traditional techniques, they present several advantages. Various minimally invasive techniques to decompress the optic nerve have been recently described. However, some include only experimental studies with no associated clinical application, and other reports describe endoscopic assistance or include techniques that require intradural procedures.14–22
Extradural optic nerve decompression through a keyhole approach may provide satisfactory decompression of the optic nerve. In this article, we propose an extradural optic nerve decompression technique through a minimally invasive approach as a modification of the method previously described by Dolenc.1,2
METHODS
The minimally invasive extradural anterior clinoidectomy (MiniEx) and minipterional craniotomy approaches for optic nerve decompression were performed using an operative microscope under magnifications of ×4 to ×25 on 4 formalin-fixed cadaveric heads. The arteries were perfused with red silicone and the veins with blue silicone. Another 2 specimens and 2 dry skulls were dissected to show the anatomic relationships among the optic nerve and its canal, the anterior clinoid process, cavernous sinus, and superior orbital fissure. The size and area of the bone flaps were measured with a caliper to avoid measurement errors.
In addition, the extradural anterior clinoidectomy approach with a MiniEx was used to decompress the optic nerve in 6 clinical cases. The surgical outcomes of these cases, including visual and neurological morbidities, were analyzed in this study.
RESULTS
Bone Relationships
The optic canal is located at the orbital apex. It is bounded by the body of the sphenoid bone medially, the lesser wing of the sphenoid bone superiorly, and the medial surface of the anterior clinoid process and optic strut laterally and the upper surface optic strut and the adjacent part of the body of the sphenoid bone below (Figure 1). The optic canal is directed backward and medially and has an oval shape in the vertical axis.23

Figure 1. Osseous relationships of the anterior clinoid process, superior orbital fissure, and optic canal. (A) Superior view. The anterior clinoid process projects backward from the medial end of the lesser wing of the sphenoid bone. The anterior attachment of the anterior clinoid process extends medially from the base of the clinoid to the planum and forms the roof of the optic canal. The posterior attachment of the anterior clinoid process, the optic strut, extends from the inferomedial aspect of the anterior clinoid to the body of the sphenoid bone and forms the inferior wall of the optic canal. Another small prominence, the middle clinoid process, situated on the medial side of the carotid sulcus at the level of the tips of the anterior clinoid process, projects upward and laterally. (B) Superior view of a left caroticoclinoid foramen. An osseous bridge extending from the tip of the anterior clinoid to the tip of the middle clinoid process creates a nearly complete bony ring around the artery, called the caroticoclinoid foramen. (C) Oblique posterior view of the left optic canal and optic strut and right superior orbital fissure. The optic canal has an oval shape and is formed superiorly by the anterior attachment of the anterior clinoid, inferiorly by the optic strut, laterally by the medial side of the anterior clinoid process and the optic strut, and medially by the sphenoid body. The superior orbital fissure has a triangular shape and is formed superiorly by the lesser wing of the sphenoid bone, medially by the optic strut and the sphenoid body, and inferiorly and laterally by the greater sphenoid wing. The maxillary strut is the bridge of bone separating the superior orbital fissure from the foramen rotundum. (D) Intraorbital view of the optic canal and superior orbital fissure. The optic strut separates the optic canal and superior orbital fissure and forms the floor of the optic canal and the superomedial part of the roof of the superior orbital fissure. Ant., anterior; Car., carotid; Caroticoclin., caroticoclinoid; Clin., clinoid; Fiss., fissure; For., foramen; Gr., greater; Inf., inferior; Less., lesser; Max., maxillary; Mid., middle; Orb., orbital; Post., posterior; Proc., process; Rotund., rotundum; Sphen., sphenoid; Sulc., sulcus; Sup., superior. (Images courtesy of AL Rhoton, Jr.)
The anterior clinoid process is a projection of bone that directs posteriorly from the medial end of the lesser wing of the sphenoid bone in the anterior part of the roof of the cavernous sinus. In a superior view, it has a triangular shape with its base located ventrally and its tip posteriorly (Figure 1A–C).24,25
The base of the anterior clinoid process has 1 lateral and 2 medial sites of attachment. Laterally, the base is attached to the lesser wing of the sphenoid bone overlying the superior orbital fissure. Medially, the base is attached through 2 roots: the anterior root extends medially from the base of the anterior clinoid process to the body of the sphenoid bone to form the roof of the optic canal and the posterior root, called the optic strut, extends medially below the optic nerve to the sphenoid body to form the floor of the optic canal (Figure 1C).
The superior surface of the optic strut forms the floor of the optic canal and its inferior surface forms the medial part of the roof of the superior orbital fissure and anterior portion of the roof of the cavernous sinus (Figure 1D). The outer layer of the anterior clinoid process is composed of dense cortical bone with an interior of cancellous bone. It may contain venous channels or may be pneumatized and include air cells that communicate with the sphenoid sinus through the optic strut. Postoperative cerebrospinal fluid leaks may occur if the sphenoid sinus is opened afterward, especially in the intradural anterior clinoidectomy or when the dura is opened after extradural anterior clinoidectomy.5,10–13,23–28
Dural Relationships
The dura that covers the superior surface of the anterior clinoid process continues medially to form the lateral part of the distal dural ring surrounding the internal carotid artery. This dura is continuous laterally with the dura that covers the superior surface of the lesser wing of the sphenoid bone. Medially, it extends below the optic nerve to include the superior surface of the optic strut and forms the anterior part of the distal dural ring. From here, the dura extends medially and posteriorly to cover the upper part of the carotid sulcus and from the medial portion of the upper ring. Anteriorly, the dura of the superior surface of the anterior clinoid process covers the anterior root of the lesser wing and attaches to the posterior edge of the planum sphenoidale (Figure 2). The clinoid segment of the internal carotid artery is located between the proximal and distal dural rings (Figures 2C and 3F).

Figure 2. Dural, arterial, and neural relationships of the optic canal, superior orbital fissure, and cavernous sinus. (A) Superolateral view of the cavernous sinus. The cavernous sinus extends from the superior orbital fissure to the petrous apex. The superior petrosal sinus passes above the ostium of the Meckel cave and joins the posterior part of the cavernous sinus. The dura covering the lateral wall has been removed, and the trigeminal ganglion has been exposed. The oculomotor, trochlear, and ophthalmic nerves pass forward to converge on the superior orbital fissure. The ophthalmic nerve has been retracted downward to expose the abducens nerve. (B) Superior view of the roof of the cavernous sinus and sellar region. The anterior clinoid process is covered by dura, which continues laterally with the dura that includes the superior aspect of the lesser wing of the sphenoid bone. The falciform ligament, the dural fold extending above the optic nerve proximal to the entrance of the nerve into the bony optic canal, extends from the base of the anterior clinoid to the tuberculum. The carotid artery exits the cavernous sinus on the medial side of the anterior clinoid process. The oculomotor nerve enters the narrow oculomotor cistern in the posterior part of the roof of the cavernous sinus referred as the oculomotor triangle. (C) Lateral view of the cavernous sinus. The anterior clinoid process has been removed, and the dural roof of the oculomotor triangle has been removed to expose the clinoid segment of the internal carotid artery in the clinoidal triangle and the posterior bend of the intracavernous carotid below the oculomotor triangle. The dura that covers the superior aspect of the clinoid continues medially around the carotid artery and forms the distal ring. The trigeminal nerve and the petrolingual ligament, extending from the petrous apex to the lingual process of the sphenoid bone, have been partially removed to expose the entrance of the petrous carotid into the cavernous sinus. The cavernous segment of the artery turns abruptly forward to course along the carotid sulcus and lateral part of the body of the sphenoid. It passes forward in a horizontal direction and terminates by moving upward along the medial side to the distal ring. The abducens nerve passes lateral to the internal carotid artery and medial to the ophthalmic nerve in the lower part of the cavernous sinus. (D–F) The relationship of the meningoperiorbital band and anterior clinoid process. (D) A right pterional craniotomy. The junction of the dura and periorbital forms the meningoperiorbital band at the lateral margin of the superior orbital fissure. (E) The anterior clinoid process has been exposed. After dividing the meningoperiorbital band, the dura of the middle fossa has to be peeled away from the anterior part of the cavernous sinus to show the anterior clinoid process. (F) Lateral exposure of the superior orbital fissure, anterior clinoid process, and cavernous sinus. The lateral edge of the superior orbital fissure (red arrow) is located anterolateral to the anterior clinoid process. After the meningoperiorbital band is divided, the dura has to be peeled posterior to the level of the interrupted vertical line to expose the anterior clinoid process for clinoidectomy. A., artery; Ant., anterior; Bas., basilar; Car., carotid; Cav., cavernous; Clin., clinoid; CN, cranial nerve; Dist., distal; Falc., falciform; Fiss., fissure; Front., frontal; Gang., ganglion; Interclin., interclinoidal; Lig., ligament; Men., meningo; Mid., middle; Oculom., oculomotor; Ophth., ophthalmic; Orb., orbital; P.C.A., posterior cerebral artery; Pet., petrosal, petrous; Petroclin., petroclinoidal; Petroling., petrolingual; Petrosphen., petrosphenoidal; Post., posterior; S.C.A., superior cerebellar artery; Seg., segment; Sup., superior; Temp., temporal; Tent., tentorial; Triang., triangle. (Images courtesy of AL Rhoton, Jr.)
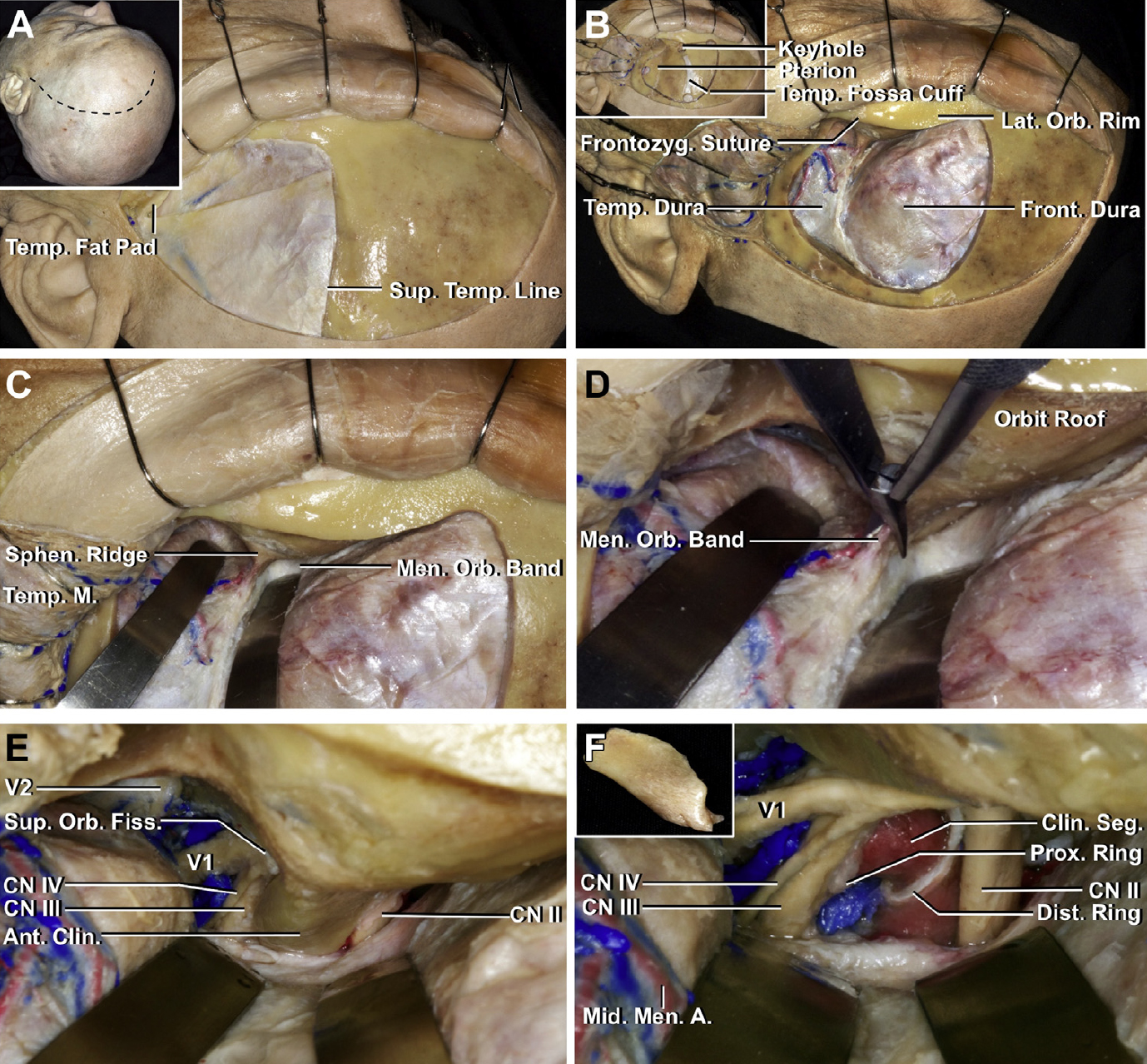
Figure 3. Surgical view of a stepwise left anterior clinoid removal and optic nerve decompression through the pterional approach. (A) The inset (upper left) show the position of the head and the site of the scalp incision. The scalp has been reflected using subgaleal dissection to expose the frontal bone and the upper part of the temporalis muscle and fascia. The facial nerve courses on the outer surface of the superficial temporal fascia above the zygomatic arch. The superficial layer of temporalis fascia has been divided just above the interfascial fat pad so that the superficial layer of temporalis fascia and the fat pad can be folded downward in continuity with the frontal pericranium to protect the branches of the facial nerve.29 (B) The inset (upper left) shows the burr holes and the craniotomy cuts for the bone flap. A cuff of temporalis fascia is preserved along the superior temporal line to aid in anchoring the temporal muscle to the line at the time of closure. The keyhole burr hole is located above and behind the frontozygomatic suture. The bone flap has been elevated to expose the temporal and frontal dura. (C) The sphenoid ridge has been flattened, and a thin shell of bone has been left along the roof and lateral wall of the orbit. The frontal and temporal dura has been retracted to expose the meningoperiorbital band at the lateral edge of the superior orbital fissure. (D) The meningo-orbital band is cut using curved microscissors. (E) The dura has been elevated from the anterior clinoid process and along the anterior wall of the cavernous sinus to expose the entrance of the oculomotor, trochlear, and ophthalmic nerves in the superior orbital fissure, and V2 in the foramen rotundum. (F) The anterior clinoid process has been removed using no-drill technique (insert) to expose the clinoid segment of the internal carotid artery between the proximal and distal dural rings. The deeper part of the optic strut has also been removed using the no-drill technique. 270° of the intercanalicular segment of the optic nerve has been decompressed. A., artery; Ant., anterior; Clin., clinoid; CN, cranial nerve., Dist., distal; Fiss., fissure; Front., frontal; Frontozyg., frontozygomatic; Lat., lateral; M., muscle; Men., meningeal, meningo; Mid., middle; Orb., Orbital; Prox., proximal; Seg., segment; Sphen., sphenoid; Sup., superior; Temp., temporal, temporalis. (Images courtesy of AL Rhoton, Jr.)
The tip of the anterior clinoid process is the site of attachment of the anteromedial tip of the tentorial edge and the anterior petroclinoid and interclinoid dural folds (Figure 2). Another dural fold, the falciform ligament, extends from the base of the clinoid across the roof of the optic canal to the planum sphenoidale (Figure 1A and B).3
Meningoperiorbital Band
The meningoperiorbital band, located at the lateral edge of the superior orbital fissure, tethers the frontotemporal basal dura to the periorbita. It blocks the elevation of the temporal dura from the lateral wall of the cavernous sinus (Figures 3C and 4G and H).
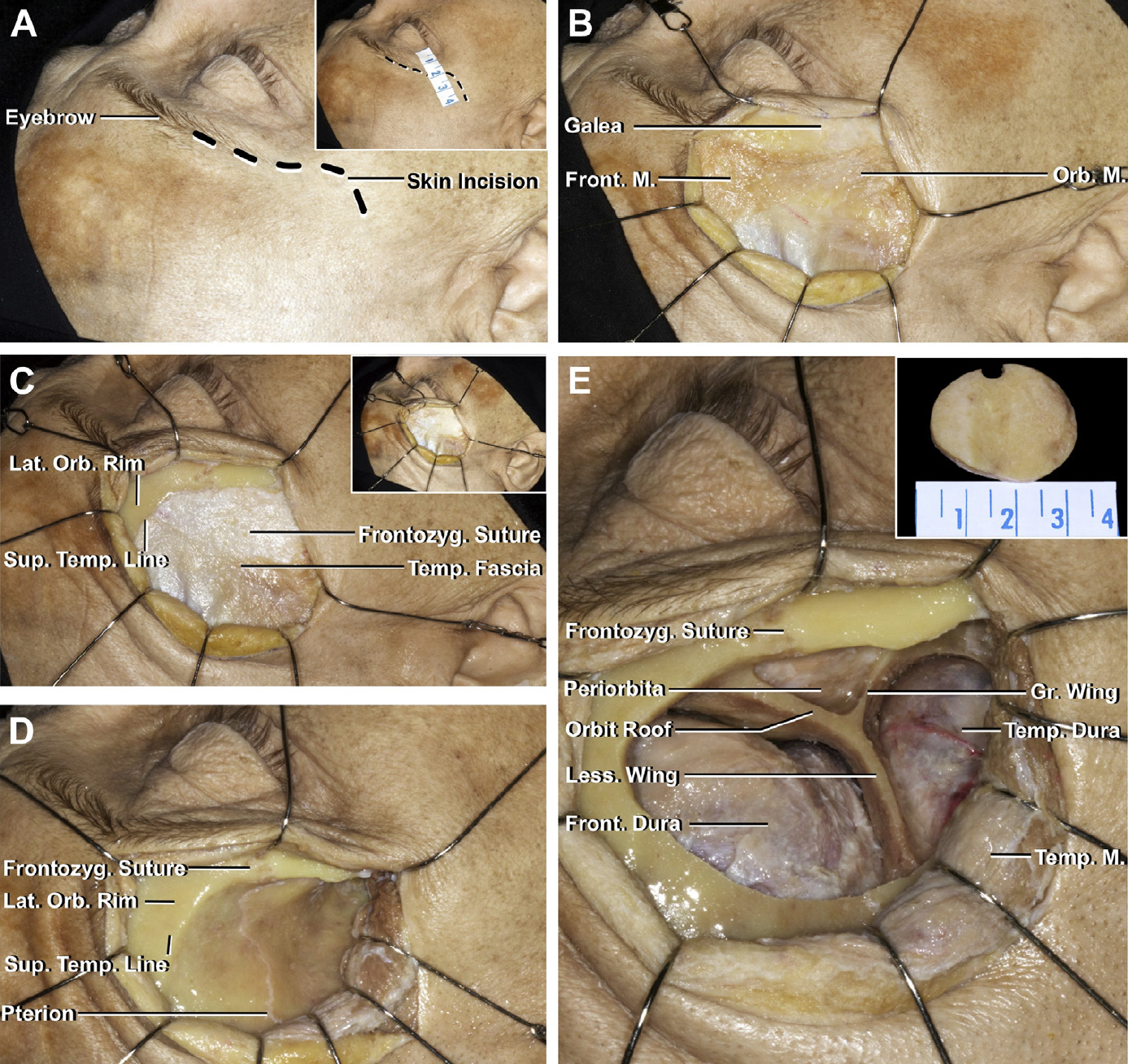
Figure 4 (A–E). Surgical views of a stepwise right optic nerve decompression through a keyhole approach. (A) Head position and the site of the scalp incision. The inset (upper right) shows the skin incision. The skin incision should avoid extending >40 mm backward from the lateral canthus to prevent the nerve to the frontalis muscle.29 It curves approximately 5 mm above the lateral orbital rim to just posterior to the lateral canthus, where it turns posteriorly in one of the horizontal skin lines just inferior to the lateral canthus. (B) The scalp has been reflected using subcutaneous dissection to expose the frontal and orbicular muscles and superficial temporal fascia. (C) Inset (upper left); the frontal muscles have been reflected superiorly and the orbitalis muscle anteriorly. The lateral orbital rim has been exposed. (D) The temporal muscle has been elevated, preserving the deep fascia, to expose the pterion and superior temporal line. (E) Bone flap or craniectomy centered at the keyhole was performed behind the frontozygomatic suture. The keyhole craniotomy exposed the frontal and temporal dura and the periorbital at a Y-shaped bone crossroad formed anteriorly and superiorly by the orbital roof, anteriorly and inferiorly by the edge of the higher wing of the sphenoid bone, and posteriorly by the lesser wing of the sphenoid bone. (Images courtesy of AL Rhoton, Jr.)
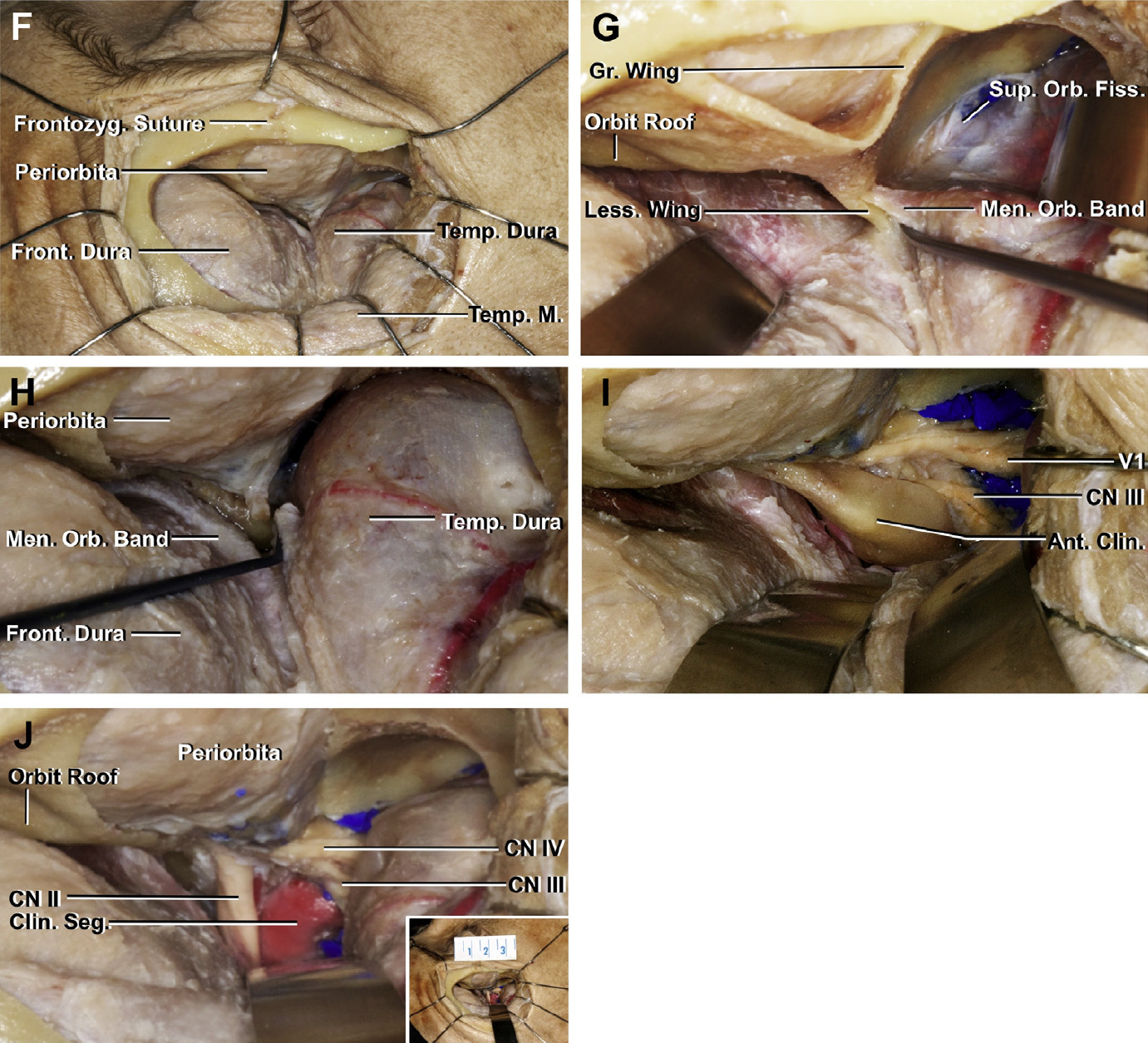
Figure 4 (F–J). Surgical views of a stepwise extradural anterior clinoidectomy and unroofing of the optic canal through the keyhole approach. (F) The lateral part of the lesser wing of the sphenoid bone was removed. (G) The frontal and temporal dura were retracted to expose the meningo-orbital band. The temporal dura was elevated to expose the superior orbital fissure. The meningo-orbital band attaches the frontotemporal basal dura to the periorbita at the level of the lateral part of the superior orbital fissure. (H) The meningo-orbital band has been cut. (I) The dura has been elevated from the anterior clinoid process and backward along the wall of the cavernous sinus to expose the entrance of the oculomotor, trochlear, and ophthalmic nerves into the superior orbital fissure. The lateral attachment of the anterior clinoid process was removed using the no-drill technique. (J) The anterior clinoid process was removed in 1 piece, and 270° of the intracanalicular portion of the optic nerve has been decompressed. The clinoid segment of the internal carotid artery has been exposed. Inset (lower right) shows that the size of the keyhole craniotomy was 3.5 cm. Ant., anterior; Clin., clinoid; CN, cranial nerve, Front., frontal, frontalis; Frontozyg., frontozygomatic; Gr., greater; Lat., lateral; Less., lesser; Men., meningo; M., muscle; Orb., orbital, orbitalis; Seg., segment; Sup., superior; Temp., temporal, temporalis. (Images courtesy of AL Rhoton, Jr.)
At the middle cranial fossa, the dura has 2 layers: periosteal and meningeal. The periosteal dura covers the bone and the meningeal dura faces the brain and covers the temporal lobe. At the superior orbital fissure, the periosteal dura exits the intracranial space and is continuous with the periorbita, whereas the meningeal layer continues intracranially. The periosteal dura joining the periorbital at the edge of the superior orbital fissure forms a strong dural band at the lateral side of the fissure that blocks elevation of the meningeal dura at this site. It is located at the outboard end of the superior orbital fissure and contains the orbitomeningeal artery and vein.10,30–34
Neural Relationships
Optic Nerve
The optic nerve is divided into 4 parts: intraocular, intraorbital, intracanalicular, and intracranial. The dural sheath around the optic nerve blends smoothly into the periorbita at the anterior end of the optic canal. After passing through the optic canal, which forms a prominence in the upper part of the sphenoid sinus immediately in front of the sella turcica and along the medial aspect of the anterior clinoid process, the intracranial portion of the nerve is directed posteriorly, superiorly, and medially toward the optic chiasm (Figure 2). The ophthalmic artery enters the orbit on the lateral side of the nerve and passes above the nerve to reach the medial sides of the orbit (Figure 2A).
Oculomotor, Trochlear, Abducens, and Ophthalmic Nerves
The oculomotor, trochlear, abducens, and ophthalmic nerves course in the inner part of the lateral wall of the cavernous sinus (Figure 2A). The abducens courses medial to the ophthalmic nerve and is adherent to the lateral surface of the intracavernous carotid medially and the medial surface of the ophthalmic nerve and the inner part of the lateral sinus wall laterally (Figure 2C).
The oculomotor nerve pierces the roof of the cavernous sinus near the center of the oculomotor triangle (Figure 2A and B), and the trochlear nerve enters the dura at the posterolateral edge of the triangle (Figure 2A). Both nerves are situated medial to and slightly beneath the level of the free edge of the tentorium at their point of entry.
The trochlear nerve enters the roof of the sinus posterolateral to the oculomotor nerve and courses below the oculomotor nerve in the posterior part of the lateral wall of the sinus. From there, the trochlear nerve passes medially between the oculomotor nerve and dura lining the lower margin of the anterior clinoid and optic strut to reach the medial part of the orbit and the superior oblique muscle (Figures 2A, 3E and F, and 4I and J).
The ophthalmic nerve is the smallest of the 3 trigeminal divisions. It is inclined upward as it passes forward near the medial surface of the dura, forming the lower part of the lateral wall of the cavernous sinus, to reach the superior orbital fissure (Figures 2A, 3E and F, and 4I and J).
The superior petrosal sinus passes above the posterior root of the trigeminal root to form the upper margin of the ostium of the Meckel cave (Figure 2A), which communicates with the subarachnoid space in the posterior fossa. The cave extends forward around the posterior trigeminal root to the midportion of the ganglion.
The abducens nerve pierces the dura, forming the lower part of the posterior wall of the cavernous sinus at the upper border of the petrous apex and enters a dural canal, referred to as the Dorello canal, where it passes below the petrosphenoid ligament (Gruber ligament). The nerve bends laterally around the proximal portion of the intracavernous carotid and gently ascends as it passes forward inside the cavernous sinus medial to the ophthalmic nerve, on the lateral side of the internal carotid artery, and below and medial to the nasociliary nerve (Figure 2A and C).28
Arterial Relationships
The cavernous segment (C3) of the internal carotid artery enters the cavernous sinus by passing medial to the petrolingual ligament and ends at the distal dural ring.27 Through its course, the cavernous segment of the internal carotid artery is divided into the posterior ascending segment, posterior curve, horizontal segment, anterior curve, and anterior ascending segment (Figure 2C).28
The segment of the internal carotid artery included between the proximal and distal dural rings is called the clinoid segment and can be exposed by removing the anterior clinoid process (Figures 2C, 3F, and 4J).28,35 The ophthalmic artery is the first branch of the supraclinoid segment of the internal carotid artery, arising just distal to the distal dural ring on the superior surface of the internal carotid artery, then coursing forward and laterally to reach the optic canal (Figure 1A).28
Extradural Anterior Clinoidectomy Through MiniEx
Position of the Head, Skin Incision, and Muscle Dissection
This approach may be implemented as part of a more complicated surgery or as a single surgical procedure. The position of the head, skin incision, and muscle dissection may vary.34 It extends from the lateral end of the eyebrow to the orbital rim just lateral to the canthus of the eye, then turns and extends posteriorly (Figure 4A).34 At the axial level of the lateral canthus of the eye, the branches of the facial nerve that innervate the orbicularis and frontalis muscles were located at a mean distance of 40.4 mm (range, 35.2–45.6 mm) above the lateral canthus of the eye.5 So, the skin incision should not extend >40 mm from the lateral canthus to avoid frontal branch injury (Figure 4A).
After the skin incision and the flap was reflected, the frontalis muscle was reflected superiorly and the orbicularis muscle inferiorly. The periosteum was incised to expose the orbital rim and the anterior and superior attachments of the temporal muscles (Figure 4B and C).36 The temporal muscle was detached from the anterior part of the superior temporal line and zygomatic and frontal processes of the frontal and zygomatic bones. Its periosteum underlying the muscle was elevated from the bone, and the muscles were reflected posteriorly and inferiorly (Figure 4D). Care should be taken to preserve the deep temporal fascia through which the deep temporal vessels and nerves that supply the muscle course to avoid temporal muscle atrophy.37,38
Extradural Stage
After the bone was exposed, a small craniotomy, 35 mm in diameter, was performed to present the frontal dura superiorly, temporal dura inferiorly, and periorbita anteriorly with a Y-shaped osseous configuration separating them (Figure 4E). We call this area “the bone crossroad.” It is formed anteriorly and superiorly by the orbital roof, anteriorly and inferiorly by the edge of a greater wing of the sphenoid bone, and posteriorly by the lesser wing of the sphenoid bone (Figure 4E). The decision as to whether to do a craniotomy or craniectomy depends on the pathology.
The frontal and temporal dura was retracted, and the lesser wing and part of the superior and lateral wall of the orbit were drilled to expose the meningo-orbital band, which was divided using curved microscissors, and the dura was elevated from the superior and inferior aspects of the anterior clinoid process from the base to the tip (Figure 4F–H). The periosteal dural layer covering the superior orbital fissure and the anterior part of the lateral wall of the cavernous sinus was elevated to expose the lateral and inferior sides of the anterior clinoid process (Figure 4I).39 The procedure continues similarly to the conventional approach. The 3 osseous attachments of the anterior clinoid process were cut using the no-drill technique using microrongeurs and the optic nerve sheath was opened (Figure 4J). Care should be taken to avoid injury of the ophthalmic artery. The incision of the optic nerve sheath should extend along its superior aspect. This strategy allows decompression of 270° of the optic nerve.
Clinical Series of Extradural Anterior Clinoidectomy Through Keyhole Approach
Six patients, 3 female, with an average age of 36.6 years (range, 7–57 years) were included in this study. Three patients had meningiomas of the tuberculum sellae, 2 patients had fibrous dysplasia, and 1 patient had a tumor in the cavernous sinus. The average surgical time for the 6 patients was 5.1 hours. The average length of stay in the intensive care unit was 1.4 days (range, 1–3 days). A bilateral procedure was performed on 3 patients. The average diameter of the craniotomy was 26.1 mm (range, 17.5–32.1 mm) and the average area was 496 mm2 (range, 349–645 mm2). The no-drill technique was used in all cases to remove the anterior clinoid process. Visual acuity was preserved in all 6 cases as shown by ophthalmologic evaluation. Only 1 patient developed bitemporal hemianopia after meningioma removal (Table 1, Figures 5 and 6).
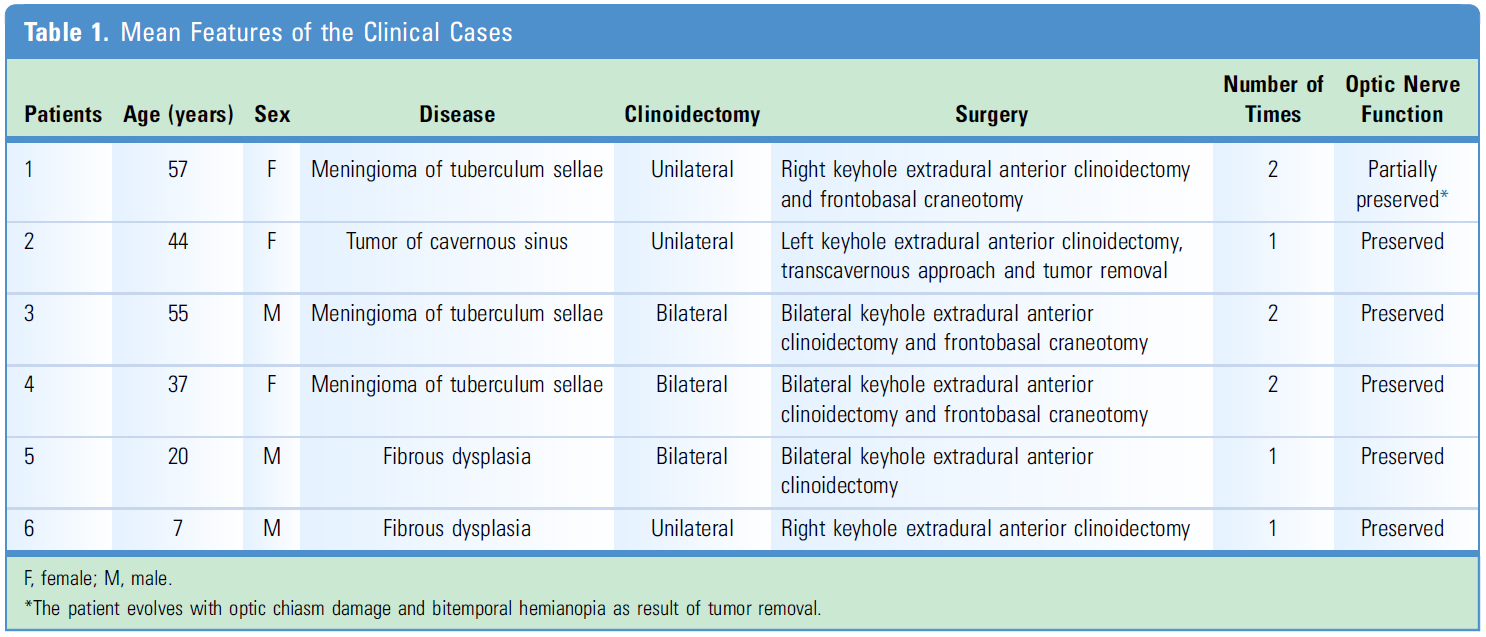

Figure 5. Illustrative case 1. Meningioma of the tuberculum sellae. A 55-year-old man, with a 1-year history of headache and progressive decrease in visual acuity. Preoperative imaging showed a tuberculum sellae meningioma. Visual fields showed right bitemporal hemianopia and left central scotoma. The procedure was performed in 2 stages. In the first, a bilateral MiniEx approach was performed to decompress the optic nerves. In the second, a subfrontal approach aimed at tumor removal. The patient had an uneventful postoperative course without complications and was discharged with improved vision. Preoperative (A) and postoperative (B) studies of a case of bilateral optic nerve decompression through a keyhole approach in a patient with a meningioma of tuberculum sellae. A coronal view of T1-weighted contrast magnetic resonance imaging study showing a tumor located at the level of the tuberculum sellae and planum that compressed both optic nerves. (B) Computed tomography with three-dimensional reconstruction, showing the bilateral keyhole, extradural anterior clinoidectomies with 270° optic nerve decompression. After bilateral optic nerve decompression, the tumor was removed through the subfrontal approach. (Images courtesy of AL Rhoton, Jr.)

Figure 6. Illustrative case 2. Fibrous dysplasia. A 7-year-old male presented with a progressive decrease in visual acuity. Preoperative imaging showed frontal-ethmoidal-sphenoidal-temporal fibrous dysplasia. Ophthalmic tests showed a reduction in right visual acuity (counting finger visual acuity). Right extradural anterior clinoidectomy through a keyhole approach was performed. In this case, obtaining a bone flap was impossible because of the fibrous dysplasia, and therefore, reconstruction was completed with a titanium plate. The patient evolved uneventfully and was discharged with improved vision. (A) Preoperative and postoperative computed tomography (CT) of right optic nerve decompression through a keyhole approach for fibrous dysplasia. An axial and coronal view of preoperative CT that showed fibrous dysplasia compressing the right optic nerve. (B) Axial and coronal postoperative CT showing the right extradural anterior clinoidectomy and optic nerve decompression through a keyhole approach. (C) Three-dimensional reconstruction of the CT showing the right keyhole approach and posterior reconstruction using a titanium plate. (Images courtesy of AL Rhoton, Jr.)
DISCUSSION
Several diseases have been associated with optic nerve compression, including fronto-orbital trauma (fracture of the optic canal with intraneural contusion or edema), intracranial tumors that involve the optic canal (meningioma of tuberculum sellae or lesser wing of the sphenoid bone or optic nerve gliomas), secondary lesions (mucocele, paranasal orbitosinusal neoplasms), fibrous or bony overgrowth, inflammatory pseudotumors, or vascular diseases (carotid-ophthalmic aneurysms)7 Optic canal involvement is common in tuberculum sellae meningiomas (77.4%) and correlates well with preoperative visual status.39
Most patients have at least some improvement in vision status after optic nerve decompression for acute or chronic compressive neuropathy.23,25,34 In cases of tumoral diseases, optic nerve decompression not only improves the visual outcome but also increases the degree of possible tumor resection.25 Early optic nerve decompression is essential for enhancing visual recovery, especially in cases of tuberculum sellae and planum sphenoidale meningiomas in which optic nerve decompression has been recommended before tumor removal.35 Margalit et al.4 concluded that early decompression of the intracanalicular optic nerve allows identification and separation of the tumor from the nerve and allows removal of them from this area with minimal manipulation of the optic nerve.
In 1985, Dolenc,1,2,33 Margalit et al.,40 and Poblete et al.38 initially described an anterior clinoidectomy via the extradural space that allows optimal mobilization of the optic nerve and the internal carotid artery. Anterior clinoidectomy facilitates tumor removal from the parasellar area and cavernous sinus as well as appropriate management of internal carotid aneurysms.33,38,40 Consequently, some modified methods have been described to accomplish safer and simpler anterior clinoidectomy.
Coscarella et al.30 reported an alternative extradural exposure of the anterior clinoid process aimed at avoiding injury of the oculomotor, lacrimal, frontal, and trigeminal nerves and their branches. Instead of exposing the anterior clinoid process from medial to lateral and dividing the meningo-orbital dural fold along the assumed safe path, they elevated the dura from the edge of the lesser wing from lateral to medial, exposed the superior orbital fissure, and peeled away the outer layer of the cavernous sinus along the greater wing medial to the foramen rotundum, to show the inferolateral surface of the anterior clinoid process. This procedure allowed dural division under full visualization to avoid damaging structures passing through the superior orbital fissure.
Minimally invasive craniotomies have increasingly become a popular alternative for traditional craniotomies in many surgical scenarios (e.g., vascular and skull base procedures). Compared with traditional techniques, they present several advantages, including less dissection of the temporal muscle, smaller bone flap, protection of neurovascular structures of the temporal muscle, preservation of the superficial temporal artery, better aesthetic outcomes, shorter surgical duration, no violation of the paranasal sinus, and reduction of the probability of damage to the cortex (Table 2). Various minimally invasive techniques to decompress the optic nerve have been recently described. However, some include only experimental studies with no associated clinical application, and other reports describe endoscopic assistance or include techniques that require intradural procedures.14–18

Abhinav et al.41 reported an endoscopic endonasal approach for optic canal decompression. They reported in an anatomic and clinical study that 160°–180° of decompression of the optic canal is technically easy to perform, but that decompression of the superolateral aspect of the optic canal to increase the extent of bony decompression to 270° is more challenging and increases risk of injury to the optic nerve.34,35,39
Rigante et al.5 described a technique of optic nerve decompression through a supraorbital approach. The maximum percentage of decompression that they accomplished was 180°. Komatsu et al.9 reported a cadaveric study of endoscopic extradural anterior clinoidectomy through a supraorbital keyhole using the high speed-drill technique. Blindness after optic canal decompression and anterior clinoidectomy has been reported. It has been attributed to the spread of heat from the drill.41 Chang28 recently described a no-drill technique of anterior clinoidectomy in which the extradural anterior clinoidectomy was performed using a small bone rongeur.
The MiniEx for optic nerve decompression through a less invasive approach may be performed as part of a more complicated surgery or aiming at only optic nerve decompression. Its small incision and minimal dissection of the temporal muscle reduces the risk of temporal muscle atrophy and cosmetic deficit compared with other techniques.41–49 This small craniotomy allows 270° decompression of the optic nerve and complete removal of the anterior clinoid process, which can be performed with drill or no-drill techniques. We prefer using the no-drill technique to avoid thermal risk to the nerve from the drill. This technique also accesses the superior orbital fissure, the clinoid segment of the carotid, and anterior part of the cavernous sinus.14,15,50,51
CONCLUSIONS
We have shown the anatomic and surgical feasibility of adequately decompressing the optic nerve through a keyhole approach. MiniEx is a novel alternative technique that allows rapid, easily reproducible, and safe decompression of the optic nerve, with a small incision and muscular dissection, reducing the cosmetic deficit. It may be carried out as part of a more complex surgery or as a single surgical procedure only for optic nerve decompression in cases of tumoral, traumatic, or chronic optic nerve compression. This study shows that MiniEx is a safe, effective, and less invasive alternative to the traditional techniques.
Contributors: Marcos Chiarullo, Jorge Mura, Pablo Rubino, Nícollas Nunes Rabelo, Rafael Martinez-Perez, Eberval Gadelha Figueiredo, and Albert L. Rhoton, Jr
Content from Chiarullo M, Mura J, Rubino P, Rabelo N, Martinez-Perez R, Figueiredo EG, Rhoton AL, Jr. Technical description of minimally invasive extradural anterior clinoidectomy and optic nerve decompression. Study of feasibility and proof of concept. World Neurosurg 2019;129:e502–e513. doi.org/10.1016/j.wneu.2019.05.196.
The Neurosurgical Atlas is honored to maintain the legacy of Albert L. Rhoton, Jr, MD.
References
- Dolenc VV. A combined epi and subdural direct approach to carotid-ophthalmic artery aneurysms. J Neurosurg. 1985;62:667-672.
- Dolenc VV. Carotid-ophthalmic aneurysms. In: Carter LP, Spetzler RF, Hamilton MG, eds. Neurovascular Surgery. New York, NY: McGraw-Hill; 1994:673-686.
- Li X, Liu M, Liu Y, Zhu S. Surgical management of tuberculum sellae meningiomas. J Clin Neurosci. 2007;14:1150-1154.
- Margalit N, Shahar T, Barkay G, et al. Tuberculum sellae meningiomas: surgical technique, visual outcome, and prognostic factors in 51 cases. J Neurol Surg B Skull Base. 2013;74:247-258.
- Rigante L, Evins AL, Berra LV, Beer-Furlan A, Stieg PE, Bernardo A. Optic nerve decompression through a supraorbital approach. J Neurol Surg B Skull Base. 2015;76:239-247.
- Bulters DO, Shenouda E, Evans BT, Mathad N, Lang DA. Visual recovery following optic nerve decompression for chronic compressive neuropathy. Acta Neurochir (Wien). 2009;151:325-334.
- Carlson AP, Stippler M, Myers O. Predictive factors for vision recovery after optic nerve decompression for chronic compressive neuropathy: systematic review and meta-analysis. J Neurol Surg B Skull Base. 2013;74:20-38.
- Galal A, Faisal A, Al-Werdany M, El Sheraby A, Lotfy T, Moharram H. Determinants of postoperative visual recovery in suprasellar meningiomas. Acta Neurochir (Wien). 2010;152:69-77.
- Komatsu F, Komatsu M, Inoue T, Tschabitscher M. Endoscopic extradural anterior clinoidectomy via supraorbital keyhole: a cadaveric study. Neurosurgery. 2011;68(2 suppl operative): 334-338.
- Noguchi A, Balasingam V, Shiokawa Y, McMenomey SO, Delashaw JB Jr. Extradural anterior clinoidectomy. Technical note. J Neurosurg. 2005;102:945-950.
- Ohta K, Yasuo K, Morikawa M, Nagashima T, Tamaki N. Treatment of tuberculum sellae meningiomas: a long-term follow-up study. J Clin Neurosci. 2001;8(suppl 1):26-31.
- Park CK, Jung HW, Yang SY, Seol HJ, Paek SH, Kim DG. Surgically treated tuberculum sellae and diaphragm sellae meningiomas: the importance of short-term visual outcome. Neurosurgery. 2006;59: 238-243.
- Schick U, Hassler W. Surgical management of tuberculum sellae meningiomas: involvement of the optic canal and visual outcome. J Neurol Neurosurg Psychiatry. 2005;76:977-983.
- Liu Y, Yu H, Zhen H. Navigation-assisted, endonasal, endoscopic optic nerve decompression for the treatment of nontraumatic optic neuropathy. J Craniomaxillofac Surg. 2019;47:328-333.
- Stähr K, Eckstein A, Holtmann L, et al. A comparative analysis of piezosurgery and oscillating saw for balanced orbital decompression [e-pub ahead of print]. Orbit. https://doi.org/10.1080/01676830.2018.1552709, accessed June 18, 2019.
- Almeida JP, Omay SB, Shetty SR, et al. Transorbital endoscopic eyelid approach for resection of sphenoorbital meningiomas with predominant hyperostosis: report of 2 cases. J Neurosurg. 2018; 128:1885-1895.
- Wang X, Wu W, Zhang H, Lan Q. Endoscopic optic nerve decompression through supraorbital keyhole extradural approach: a cadaveric study. Turk Neurosurg. 2017;27:212-216.
- Lubbe D, Mustak H, Taylor A, Fagan J. Minimally invasive endo-orbital approach to sphenoid wing meningiomas improves visual outcomes - our experience with the first seven cases. Clin Otolaryngol. 2017;42:876-880.
- Singh H, Essayed WI, Jada A, et al. Contralateral supraorbital keyhole approach to medial optic nerve lesions: an anatomoclinical study. J Neurosurg. 2017;126:940-944.
- Berhouma M, Jacquesson T, Abouaf L, Vighetto A, Jouanneau E. Endoscopic endonasal optic nerve and orbital apex decompression for nontraumatic optic neuropathy: surgical nuances and review of the literature. Neurosurg Focus. 2014;37:E19.
- Vaitheeswaran K, Kaur P, Garg S. Minimal invasive transcaruncular optic canal decompression for traumatic optic neuropathy. Orbit. 2014;33: 456-458.
- Chen F, Zuo K, Feng S, et al. A modified surgical procedure for endoscopic optic nerve decompression for the treatment of traumatic optic neuropathy. North Am J Med Sci. 2014;6:270-273.
- Cornelius CP, Mayer P, Ehrenfeld M, Metzger MC. The orbits’ anatomical features in view of innovative surgical methods. Facial Plast Surg. 2014;30:487-508.
- Kim JM, Romano A, Sanan A, van Loveren HR, Keller JT. Microsurgical anatomic features and nomenclature of the paraclinoid region. Neurosurgery. 2000;46:670-682.
- Tripathi M, Deo RC, Damodaran N, et al. Quantitative analysis of variable extent of anterior clinoidectomy with intradural and extradural approaches: 3-dimensional analysis and cadaver dissection. Neurosurgery. 2015;11(suppl 2):147-160.
- Avci E, Bademci G, Ozturk A. Microsurgical landmarks for safe removal of anterior clinoid process. Minim Invasive Neurosurg. 2005;48:268-272.
- Rhoton AL Jr. The anterior and middle cranial base. Neurosurgery. 2002;51(4 suppl):S273-S302.
- Rhoton AL Jr. The cavernous sinus, the cavernous venous plexus, and the carotid collar. Neurosurgery. 2002;51(4 suppl):S375-S410.
- Moe K, Bergeron CM, Ellenbogen RG. Transorbital neuroendoscopic surgery. Neurosurgery. 2010;67(3 suppl operative):ons16-ons28.
- Coscarella E, Baskaya M, Morcos J. An alternative extradural exposure to the anterior clinoid process: the superior orbital fissure as a surgical corridor. Neurosurgery. 2003;53:162-167.
- Froelich SC, Aziz KM, Levine NB, Theodosopoulos P, van Loveren HR, Keller JT. Refinement of the extradural anterior clinoidectomy: surgical anatomy of the orbitotemporal periosteal fold. Neurosurgery. 2007;61(5 suppl 2):179-186.
- Fukuda H, Evins AI, Burrell JC, Iwasaki K, Stieg PE, Bernardo A. The meningo-orbital band: microsurgical anatomy and surgical detachment of the membranous structures through a frontotemporal craniotomy with removal of the anterior clinoid process. J Neurol Surg B Skull Base. 2014;75:125-132.
- Dolenc VV. Frontotemporal epidural approach to trigeminal neurinomas. Acta Neurochir (Wien). 1994;130:55-65.
- Rhoton AL Jr. The sellar region. Neurosurgery. 2002;51(4 suppl):S335-S374.
- Sade B, Lee JH. High incidence of optic canal involvement in tuberculum sellae meningiomas: rationale for aggressive skull base approach. Surg Neurol. 2009;72:118-123.
- Ellis D, Stewart W. Lateral orbitotomy. In: Toth BA, Keating RF, Stewart W, eds. An Atlas of Orbitocranial Surgery. London, United Kingdom: CRC Press; 1999.
- Keyhole Approaches in Neurosurgery. In: Perneczky A, Reisch R, eds. Concept and Surgical Technique. Volume 1. Vienna, Austria: Springer; 2008:179-204.
- Poblete T, Jiang X, Komune N, Matsushima K, Rhoton AL Jr. Preservation of the nerves to the frontalis muscle during pterional craniotomy. J Neurosurg. 2015;122:1274-1282.
- Rhoton AL Jr. Aneurysms. Neurosurgery. 2002;51(4 suppl):S121-S158.
- Margalit NS, Lesser JB, Moche J, Sen C. Meningiomas involving the optic nerve: technical aspects and outcomes for a series of 50 patients. Neurosurgery. 2003;53:523-533.
- Mathiesen T, Kihlström L. Visual outcome of tuberculum sellae meningiomas after extradural optic nerve decompression. Neurosurgery. 2006;59:570-576.
- Nozaki K, Kikuta K, Takagi Y, Mineharu Y, Takahashi J, Hashimoto N. Effect of early optic canal unroofing on the outcome of visual functions in surgery for meningiomas of the tuberculum sellae and planum sphenoidale. Neurosurgery. 2008;62:839-844.
- Chang DJ. The “no- drill” technique of anterior clinoidectomy: a cranial base approach to the paraclinoid and parasellar region. Neurosurgery. 2009;64(3 suppl):96-106.
- Wen HT, de Oliveira E, Tedeschi H, Andrade FC, Rhoton AL Jr. The pterional approach: surgical anatomy, operative technique, and rationale. Operat Tech Neurosurg. 2001;4:60-72.
- Yang Y, Wang H, Shao Y, Wei Z, Zhu S, Wang J. Extradural anterior clinoidectomy as an alternative approach for optic nerve decompression: anatomic study and clinical experience. Neurosurgery. 2006;59(4 suppl 2):ONS253-ONS262.
- Yaşargil MG, Reichman MV, Kubik S. Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. J Neurosurg. 1987;67:464-466.
- Yaşargil MG. Interfascial pterional (frontotemporosphenoidal) craniotomy. In: Yaşargil MG, ed. Microneurosurgery. 1. Stuttgart: Georg Thieme Verlag; 1984:215-220.
- Rhoton AL Jr. The orbit. Neurosurgery. 2002;51(4 suppl):S303-S334.
- Figueiredo EG, Deshmukh P, Nakaji P, et al. The minipterional craniotomy: technical description and anatomic assessment. Neurosurgery. 2007;61(5 suppl 2):256-264.
- Figueiredo EG, Welling LC, Preul MC, et al. Surgical experience of minipterional craniotomy with 102 ruptured and unruptured anterior circulation aneurysms. J Clin Neurosci. 2016;27:34-39.
- Welling LC, Figueiredo EG, Wen HT, et al. Prospective randomized study comparing clinical, functional, and aesthetic results of minipterional and classic pterional craniotomies. J Neurosurg. 2015;122:1012-1019.
Please login to post a comment.




