

Neurofibromatosis Type 1

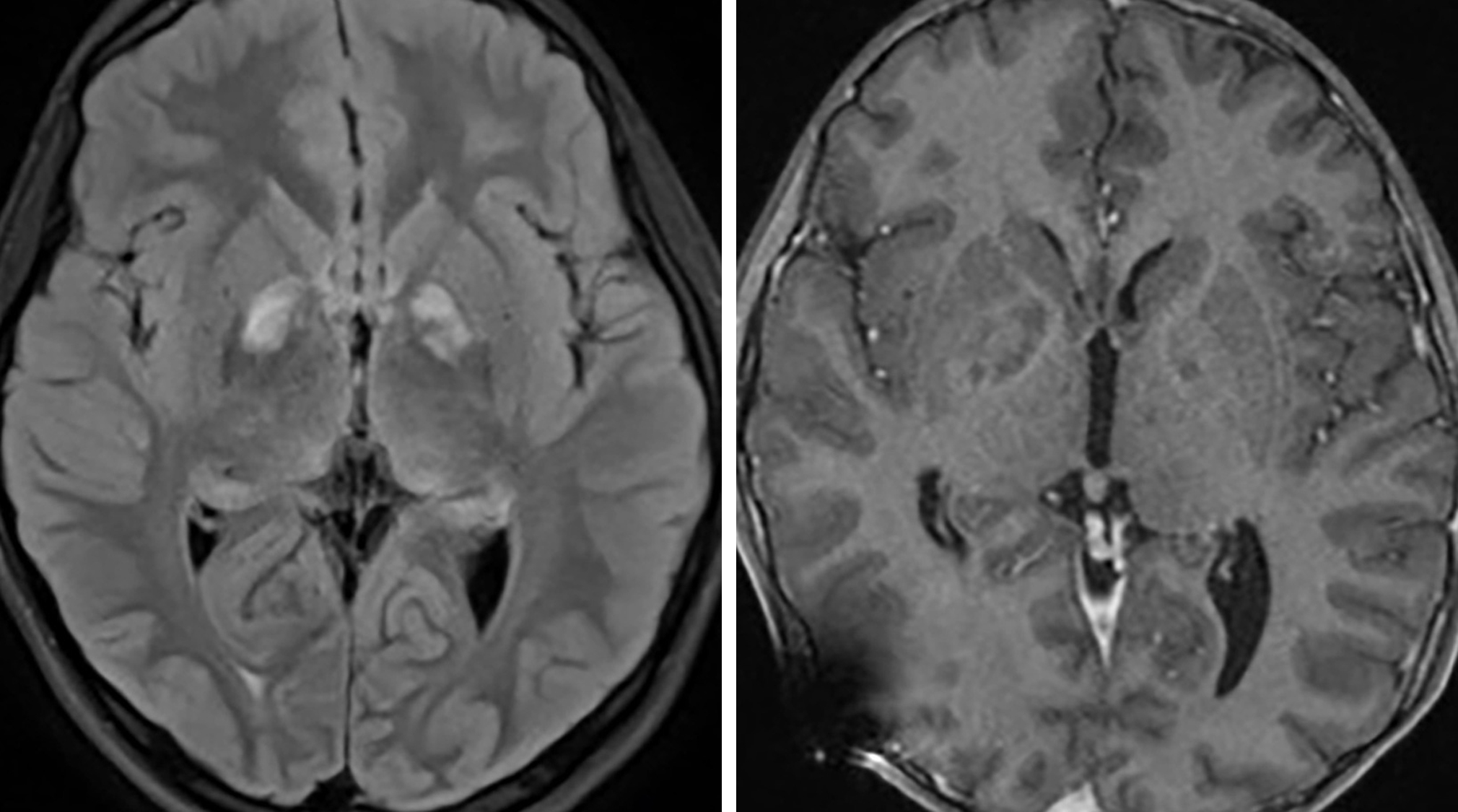
Figure 1: Though associated with many tumors, these NF lesions are merely tumor mimics. Notice the FLAIR-hyperintense (left) nonenhancing (right) abnormalities within the globus pallidus and, to a lesser extent, the dorsal thalami, compatible with FASI. These regions can be seen in the basal ganglia, thalami, brainstem, cerebellum, or subcortical white matter.

Figure 2: Axial FLAIR images through the basal ganglia (top left) and pons (top right) demonstrate expansile hyperintense lesions most compatible with NF dysplasias, a tumor mimic. Low-grade tumors may also be present with NF1, including optic nerve glioma, seen as right-greater-than-left optic nerve enlargement on coronal T2FS (bottom left) and sagittal T1 postcontrast (bottom right) images.
Description
- Multisystem neurocutaneous disorder with variable expression but 100% penetrance
- Most common phacomatosis, occurring in 1 of 2000 live births
- 50% are inherited as an autosomal dominant condition, whereas the other 50% are a result of a new mutation

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
Pathology
- Neurofibromatosis type 1 (NF1) gene locus is on chromosome 17q11.2
- Gene product is neurofibromin 1, which normally functions as a tumor suppressor
Clinical Features
- Symptoms
- Highly variable
- Diagnosis requires ≥2 of the following
- > 6 café au lait spots
- ≥2 neurofibromas
- 1 plexiform neurofibroma
- Optic nerve glioma
- Sphenoid wing dysplasia
- Lisch nodules
- Axillary or inguinal freckles
- Primary relative with NF1
- Often have associated learning disabilities
- Age
- 50% meet the criteria by 1 year of age
- 95% meet the criteria by 8 years of age
- Gender
- No gender predilection
Imaging
- Findings highly variable with multisystem involvement
- CNS findings
- Optic nerve glioma
- CT
- Fusiform or exophytic enlargement and enhancement with associated kinking or buckling
- MRI
- T1WI
- Hypointense to isointense enlargement
- T2WI
- Hyperintense centrally, hypointense along the periphery
- Contrast
- Variable enhancement
- T1WI
- CT
- Focal areas of signal intensity (FASI)
- Identified in the basal ganglia, thalamus, brainstem, cerebellum, and subcortical white matter; no associated mass effect
- Usually resolve or decrease with age
- CT
- Normal
- MRI
- T1WI
- Isointense to slightly hyperintense
- T2WI
- Hyperintense
- Enhancement
- None
- T1WI
- MR spectroscopy
- Usually normal
- Sphenoid wing dysplasia
- Can be isolated or associated with underlying plexiform neurofibroma
- CT is the most effective imaging modality
- Moyamoya disease
- A rare finding in NF1
- CT
- Atrophy most notable anteriorly
- May have associated hemorrhage
- CT angiography
- Attenuated, abnormal circle of Willis with net-like collaterals
- MRI
- T1WI
- Multiple dot-like flow voids in the basal ganglia
- T2WI
- Hyperintense lacunar infarcts
- T2*/SWI/GRE
- Hypointense signal if previous hemorrhage
- DWI
- Reduced diffusivity in regions of acute infarction
- Contrast
- Enhancing dots in basal ganglia with associated leptomeningeal enhancement
- T1WI
- Optic nerve glioma
- Imaging recommendations
- MRI of brain and orbits with contrast
- Mimic
- Many tumor types are present in patients with NF1 (optic gliomas, neurofibromas); FASI are not true neoplasms and are usually easily distinguished from neoplasms by their typical locations, signal intensities, and tendency to involute over time
For more information, please see the corresponding chapter in Radiopaedia.
Contributor: Sean Dodson, MD, and Jacob A. Eitel, MD
References
Aoki S, Barkovich AJ, Nishimura K, et al. Neurofibromatosis types 1 and 2: cranial MR findings. Radiology 1989;172:527–534. doi.org/10.1148/radiology.172.2.2501822
Fortman BJ, Kuszyk BS, Urban BA, et al. Neurofibromatosis type 1: a diagnostic mimicker at CT. Radiographics 2001;21:601–612. doi.org/10.1148/radiographics.21.3.g01ma05601
Van Es S, North KN, McHugh K,et al. MRI findings in children with neurofibromatosis type 1: a prospective study. Pediatr Radiol 1996;26:478–487. doi.org/10.1007/BF01377205
Please login to post a comment.



