

Oculomotor Nerve

ABSTRACT
The oculomotor nerve supplies the extraocular muscles. It also supplies the ciliary and sphincter pupillae muscles through the ciliary ganglion. The nerve fibers leave the midbrain through the most medial part of the cerebral peduncle and enter the interpeduncular cistern. After the oculomotor nerve emerges from the interpeduncular fossa, it enters the cavernous sinus slightly lateral and anterior to the dorsum sellae. It enters the orbit through the superior orbital fissure, after exiting the cavernous sinus, to innervate the extraocular muscles. Therefore, knowledge of the detailed anatomy and pathway of the oculomotor nerve is critical for the management of lesions located in the middle cranial fossa and the clival, cavernous, and orbital regions. This review describes the microsurgical anatomy of the oculomotor nerve and presents pictures illustrating this nerve and its surrounding connective and neurovascular structures.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
INTRODUCTION
The oculomotor nerve is a pure motor nerve and primarily triggers movements of the eyeball, hence its name (from the Latin oculus for eye and motous for motion) (Dorland, 2003). It contains general somatic efferent fibers that move the eyeball and general visceral efferent fibers that constrict the pupil and control accommodation (Gould and Fix, 2014). It supplies all the extraocular muscles except the superior oblique and lateral rectus and also innervates the sphincter pupillae and ciliary muscles. It can be divided into seven segments: intramesencephalic, interpeduncular cisternal, petroclinoid, trigonal, cavernous, fissural, and orbital (Fig. 1).

Figure 1. A: Schematic lateral view of the left ONC and trochlear nerve. The Edinger–Westphal nucleus is rostral to the caudal central nucleus and mainly dorsal to the lateral somatic cell columns. B: Schematic superior view of the ONC and trochlear nerve. The medial cell nucleus is medial to both the dorsal and intermediate cell nuclei. C: Schematic posterolateral view of the brain stem. The ONC is positioned in the most ventral part of the periaqueductal gray at the level of the superior colliculus. The trochlear nucleus is in the ventral gray matter near the midline at the level of the inferior colliculus. D: Schematic view of lateral somatic cell columns containing motor neuron for the extraocular muscles innervation. E: Superolateral view of the right oculomotor nerve from the cisternal segment to the orbital segment. The oculomotor nerve can be divided into seven segments: intramesencephalic, interpeduncular cisternal, petroclinoid, trigonal, cavernous, fissural, and orbital. Abbreviations: EW, Edinger–Westphal; Inf., inferior; Sup., superior. (Images courtesy of AL Rhoton, Jr.)
INTRAMESENCEPHALIC SEGMENT
The intramesencephalic segment extends from the nucleus to the point of exit of the oculomotor nerve from the midbrain. The oculomotor nuclear complex (ONC) and the initial parts of the nerve fibers are located within the tegmentum of the midbrain, which is in turn situated at the level of the tentorial notch, where it is surrounded by parts of the diencephalon, cerebellum, and cerebral hemisphere (Parent and Carpenter, 1995). The oculomotor nerve complex, which is positioned in the most ventral part of the periaqueductal gray (PAG) at the level of the superior colliculi, comprises the somatic cell column, the Edinger–Westphal nucleus, and an additional dorsal (supraoculomotor) nucleus in each half of the midbrain (Figs. 1A–1C) (Vitosevic et al., 2013). The somatic cell columns are divided into large lateral and small central caudal columns (central caudal nucleus) (Figs. 1A and 1B).
The large lateral somatic cell columns contain motor neurons that innervate the extraocular muscles. The dorsal cell column (nucleus) innervates the inferior rectus muscle, the intermediate cell column (nucleus) innervates the inferior oblique muscle, and the ventral cell column (nucleus) supplies fibers to the medial rectus muscle. The fibers arising from these cell columns are uncrossed. However, a cell column medial to both the dorsal and intermediate cell columns, referred to as the medial cell column, provides crossed fibers that innervate the superior rectus muscle (Fig. 1D) (Horn et al., 2008; Parent and Carpenter, 1995; Vitosevic et al., 2013).
The caudal central nucleus is a midline somatic cell group found only in the caudal third of the complex. It gives rise to crossed and uncrossed fibers that innervate the levator palpebrae superior muscles (Fig. 1D) (Parent and Carpenter, 1995; Gould and Fix, 2014).
The Edinger–Westphal (EW) nucleus extends along the raphe, rostral to the caudal central nucleus and mainly dorsal to the lateral somatic columns (Figs. 1A and 1B). It contains some of the neurons that innervate the sphincter pupillae muscle and the ciliary muscle (accommodation fibers) in certain animals. However, in humans, these preganglionic parasympathetic neurons are located in a small cell collection just dorsal to the classical EW nucleus (Buttner-Ennever, 2006; Horn et al., 2008; May et al., 2008; Kozicz et al., 2011). The EW nucleus contains many neurons that send axons not to the ciliary ganglion but to the spinal cord, the lower part of the brainstem, and the cerebellum(Loewy et al., 1978; Sugimoto et al., 1978; Clarke et al., 1985). The function of these connections is unknown.
Lesions of the ONC can be unilateral or bilateral, complete or partial. A complete lesion usually results in total ipsilateral ophthalmoplegia, an elevation paresis of the opposite eye, bilateral ptosis, and ipsilateral mydriasis (Biller et al., 1984). A partial ophthalmoplegia can be due to a lesion in any part of the oculomotor complex in the rostrocaudal direction. Most of the fascicles arising from the ONC course ventrolaterally and diverge through the medial longitudinal fasciculus (MLF). They form much of the larger extranuclear tegmental fascicles of the oculomotor nerve. According to a recent study by Vitosevic et al. three groups of these fascicles can be distinguished along their course from the MLF to the interpeduncular cistern in a caudal-to-rostral direction: the caudal, intermediate, and rostral (Vitosevic et al., 2013).
A rostrocaudal topographical arrangement of specific oculomotor fascicles has been proposed (Ksiazek et al., 1994; Saeki et al., 2000). The caudal fascicles, which most likely innervate the superior rectus and the levator palpebrae muscles, extend through the superior cerebellar peduncle just caudal to the red nucleus and close to the lateral lemniscus. The intermediate fascicles, which innervate the medial rectus and the inferior oblique muscles, always pass through the superior cerebellar peduncle, either just medial to the caudal part of the red nucleus (60%), or, less frequently (40%), through the nucleus itself. The rostral oculomotor fascicles, which terminate in the inferior rectus and sphincter pupillae muscles, course medial to the rostral part of the red nucleus (Ksiazek et al., 1994; Vitosevic et al., 2013).
A model of the oculomotor fascicular organization has also been proposed in the transverse (medial-to-lateral) direction (Castro et al., 1990; Brazis et al., 2001). Thus, the pupilloconstrictor fibers occupy the most medial area in the transverse plane, close to the interpeduncular cistern. Somewhat laterally lie the inferior rectus fibers, and more laterally the medial rectus and lid elevators fibers. The most lateral fascicles innervate the superior rectus and inferior oblique muscles. This organization also implies the possibility of isolated injury to the nerve fibers of individual extraocular muscles or their various combinations (Ford et al., 1984; Parent and Carpenter, 1995; Purvin, 2010). The oculomotor nerve fascicles converge in a posterior-to-anterior direction, leave the midbrain through the most medial part of the cerebral peduncle, and enter the interpeduncular cistern.
The vascular supply to the oculomotor nuclei and fascicles is via a median group of arteries that arise from the terminal bifurcation of the basilar artery at the origin of the superior cerebellar and posterior cerebral arteries (Porter and Baker, 1998). These arteries enter the brainstem through the interpeduncular fossa and course dorsally, producing a dense bundle to supply the midline structures up to and along the floor of the cerebral aqueduct (Fig. 2A).
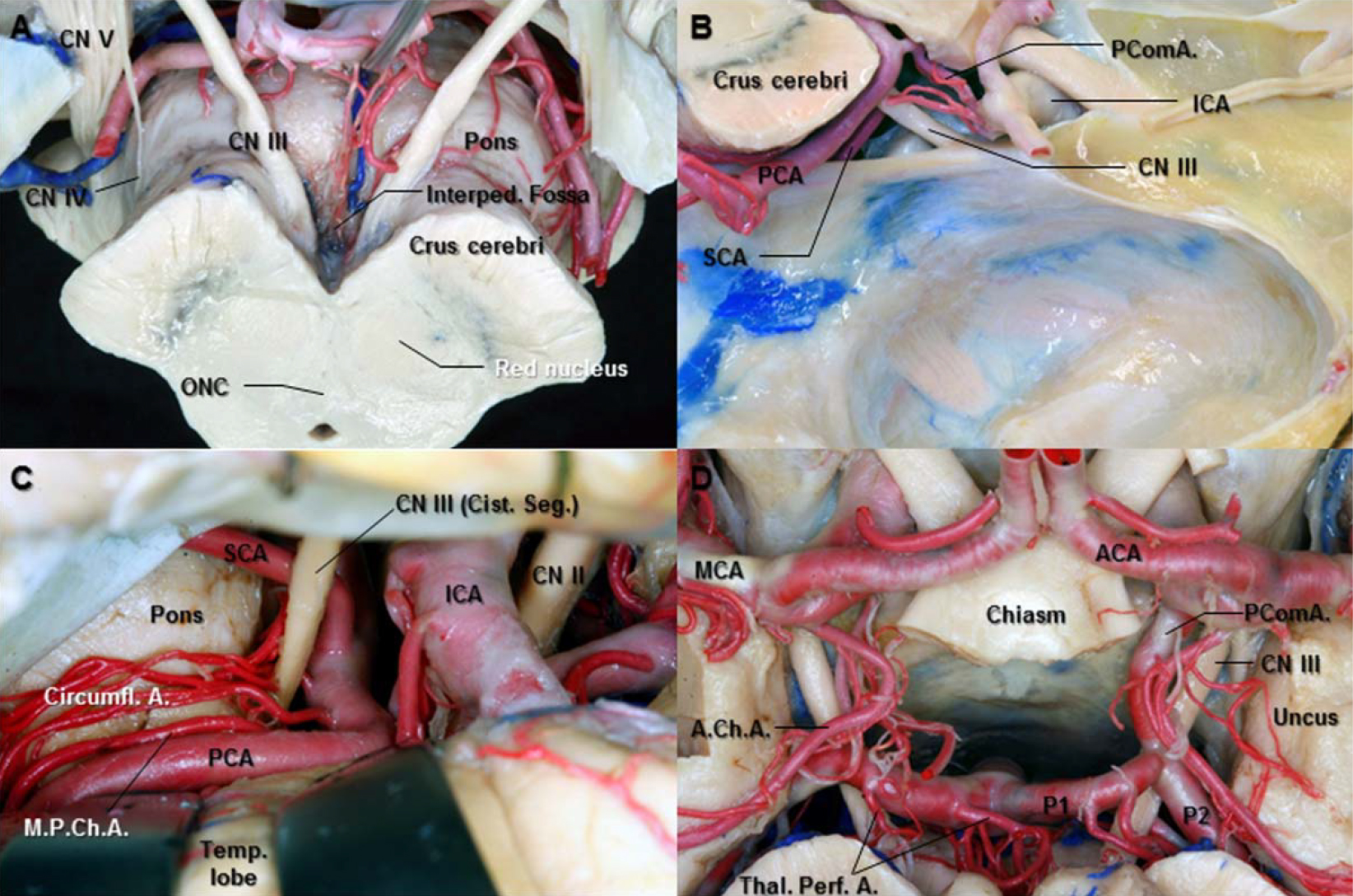
Figure 2. A: Superior and anterior view of the midbrain and pons. The oculomotor nerve originates in the middle part of the cerebral peduncle at the medial side. The cisternal segment passes through the interpeduncular cistern inferiorly, anteriorly, and laterally. B: The cisternal segment of the oculomotor nerve courses between the PCA superiorly and the SCA inferiorly in the anterior incisural space. C: The left subtemporal approach (retraction of the temporal lobe) shows the oculomotor nerve passing between the PCA and the SCA. D: Superior view of the circle of Willis. The oculomotor nerve passes inferomedial to the uncus and inferolateral to the PComA. Abbreviations: A., artery; ACA., anterior cerebral artery; A.Ch.A., anterior choroidal artery; Circumfl., circumflex; Cist., cisternal; CN., cranial nerve; ICA., internal carotid artery; Interped., interpeduncular; MCA., middle cerebral artery; M.P.Ch.A., medial posterior choroidal artery; ONC., oculomotor nuclear complex; PComA., posterior communicating artery; PCA., posterior cerebral artery; P1., precommunicating segment of the PCA; P2., postcommunicating segment of the PCA; SCA., superior cerebellar artery; Seg., segment; Temp., temporal; Thal. Perf. A., thalamoperforating artery. (Images courtesy of AL Rhoton, Jr.)
INTERPEDUNCULAR CISTERNAL SEGMENT
The oculomotor nerve originates in the middle part of the cerebral peduncle at the medial side. The cisternal segment then passes through the interpeduncular cistern inferiorly, anteriorly, and laterally (Fig. 2A) (Liang et al., 2009). The interpeduncular cistern, which sits in the posterior part of the anterior incisural space between the cerebral peduncles and the dorsum sellae, communicates laterally with the sylvian cistern below the anterior perforated substance and anteriorly with the chiasmatic cistern below the optic chiasm. Some of the nerve roots arise from the middle or the inner portion of the cerebral peduncle. Generally, the rootlets of the oculomotor nerve immediately unite and extend as a single root (Margolis et al., 1974). The cisternal segment extends from the exit point of the nerve in the medial side of the cerebral peduncle to the posterior petroclinoid fold, the posterior margin of the oculomotor triangle (Figs. 2A and 2B).
The oculomotor nerve courses between the posterior cerebral artery (PCA) superiorly and superior cerebellar artery (SCA) inferiorly in the anterior incisural space. It is therefore a good landmark for identifying the PCA and SCA (Figs. 2B and 2C). It passes inferomedial to the uncus and inferolateral to the posterior communicating artery (PComA) to enter the roof of the cavernous sinus through the oculomotor trigone. However, if the PComA remains as the major origin of the PCA, termed the fetal type of PComA, it courses further laterally above or lateral to the oculomotor nerve (Figs. 2C and 2D) (Rhoton, 2002b). At the middle part of the cisternal segment, the oculomotor nerve keeps close to the uncus between the PComA and uncus and runs parallel to the PComA. Its mean distance from the PComA is 1.7 ± 0.4 mm, and its mean diameter at the middle part of the cisternal segment is 2.14 ± 0.2 mm. The maximum visualized length from its exit point to its dural entry point is 14.61 ± 2.33 mm. The angle between the oculomotor nerve and median sagittal plane is 24.48° ± 4.57° on the left and 24.48° ± 5.07° on the right (Liang et al., 2009). The oculomotor nerve has a long intracranial course and a very narrow diameter, so it is fragile and subject to injury resulting from tumor growth, trauma, infection, and aneurysm formation, and can easily be injured by surgical manipulation at the incision. Patients can present with an isolated or non-isolated, pupil-sparing or non-pupil-sparing, oculomotor nerve palsy. These clinical features are useful for locating the lesion along the course of the nerve and establishing its most likely cause, so the choice of diagnostic tests should be based on the clinical features of the palsy (Hashimoto et al., 1998; Albayram et al., 2006).
Although the subarachnoid or cisternal portion of the oculomotor nerve is a single structure, and previous clinical observations indicate a topographic arrangement of the fibers within the nerve, the precise anatomical arrangement in humans has not been specified. The few localization studies in animals have demonstrated that pupillary fibers are superficially located in the cisternal portion of the oculomotor nerve (Atasever et al., 1993; Srinivasan et al., 2015). Fixed dilated pupils strongly suggest oculomotor nerve compression, the most common causes of which are aneurysm (especially in the PComA), trauma, and an intracranial mass lesion. When the peripheral oculomotor nerve is involved by a mass lesion or aneurysm, the pupilloconstricter fibers are usually involved first, followed in order by palsy of the levator palpebrae, superior rectus, and medial rectus (Srinivasan et al., 2015). In contrast, pupil-sparing palsy of the oculomotor nerve is a hallmark of an ischemic lesion, which tends to involve the central core of the nerve. The most common cause is likely to be an ischemic process affecting the oculomotor nerve or the midbrain (Miyazaki, 1985; Trobe, 1988; Liang et al., 2009).
The relationship between the cisternal segment of the oculomotor nerve and the PCA and SCA has been studied extensively. The proximal portion of this segment is closely related to segment P1 and the thalamoperforating, collicular, and short circumferential arteries, but the distal portion is close to segment P2 and the medial posterior choroidal arteries (Figs. 2C and 2D). Therefore, compression of this part of the artery can cause dysfunction of the intraneural circulation and ischemia of the nerve. A lesion of the main artery (PCA or basilar artery) can cause complete paralysis of the nerve (Madonick and Ruskin, 1962; Caruso et al., 1991; Goto et al., 1993; Uz and Tekdemir, 2006).
After leaving the midbrain, the oculomotor nerve courses anterolaterally in the interpeduncular cistern and then pierces the cistern. Liliequist’s membrane, separating the chiasmatic, interpeduncular and prepontine cisterns, courses as a continuation of the basal arachnoid membrane over the posterior clinoid and splits into the diencephalic and mesencephalic leaves. The lateral attachment of the diencephalic leaf is related to the arachnoid sheath surrounding the oculomotor nerve, with numerous trabeculae extending from the oculomotor nerve to the uncus and tentorium (Anik et al., 2011; Wang et al., 2011; Mortazavi et al., 2015). Therefore, in cases where the oculomotor nerve is to be mobilized to widen the carotid-oculomotor window, full dissection of the arachnoid sleeve surrounding the nerve is required (Fig. 2C) (Froelich et al., 2008).
PETROCLINOID SEGMENT
The petroclinoid segment of the oculomotor nerve is located between the cisternal and trigonal segments. It is proximal to the oculomotor porus, located in the roof of the cavernous sinus near the center of the oculomotor triangle (Figs. 3A and 3B). It is limited posteriorly by the posterior petroclinoid fold and anteriorly by the oculomotor porus of the roof of the cavernous sinus (Figs. 3A–3C). Therefore, the oculomotor triangle represents the floor of the petroclinoid segment. The length and diameter of this segment average 4.9 mm (range, 3.6–6.2 mm) and 2.3 mm (range, 1.7–2.9 mm), respectively (Iaconetta et al., 2010). Lesions invading the cavernous sinus from the parasellar region are most likely to cause oculomotor nerve dysfunction before the other cranial nerves within the cavernous sinus become involved. This is probably because of the close proximity of the nerve to the unyielding interclinoid ligament above and the petroclinoid dural folds below it (Hall et al., 1983; Cano et al., 1989; Iaconetta et al., 2010). Also, this segment can be especially vulnerable when the brainstem shifts downward at the moment of head injury. The mechanisms of nerve injury can be ascribed to partial tearing of the parasympathetic fibers contused against the posterior clinoid or the petroclinoid ligament (Figs. 3A and 3C) (Mariak et al. 1997; Aygun et al., 2005; Kraus et al., 2007). Care should be taken to preserve this segment during posterior clinoid drilling to facilitate entry to the posterior fossa and clival areas (Fig. 3B).

Figure 3. A: The cisternal segment of the oculomotor nerve extends from the exit point of the nerve in the medial side of the cerebral peduncle to the posterior petroclinoid fold, the posterior margin of the oculomotor triangle. B: The left transslyvian approach exposes the cisternal segment of the oculomotor nerve after retraction of the ICA to the medial side. C: The petroclinoid segment of the oculomotor nerve is located between the cisternal and trigonal segments. The petroclinoid segment ends at the oculomotor porus. The dura forming the oculomotor porus has been incised and retracted to the lateral side. The trigonal segment of the oculomotor nerve has been exposed. An impression on the upper surface of the nerve is commonly observed at the level of the porus. D: The superficial layer of the lateral wall of the cavernous sinus has been removed to expose the trigonal segment of the oculomotor nerve, oculomotor cistern, and trigeminal nerve. Abbreviations: ACP., anterior clinoid process; BA., basilar artery; CN., cranial nerve; CS., cavernous sinus; ICA., internal carotid artery; Lat., lateral; Lig., ligament; MCA., middle cerebral artery; Oculom. Triang, oculomotor triangle; PCA., posterior cerebral artery; PCP., posterior clinoid process; Petroclin., petroclinoid; Post., posterior; SCA., superior cerebellar artery; Seg., segment. (Images courtesy of AL Rhoton, Jr.)
TRIGONAL SEGMENT
The petroclinoid segment ends at the oculomotor porus where the nerve pierces the roof of the cavernous sinus, entering near the center of the oculomotor triangle (Fig. 3). The anterior petroclinoid dural fold, an anterior extension of the tentorial edge, extends from the anterior clinoid process to the petrous apex and forms the lateral margin of the oculomotor triangle. The medial edge of the oculomotor triangle is formed by the interclinoid ligament, which extends from the anterior to the posterior clinoid process, and its posterior edge is formed by the posterior petroclinoid fold, which extends from the posterior clinoid process to the petrous apex (Martins et al., 2006). The oculomotor cistern, a CSF-filled arachnoid and dural cuff, begins at the oculomotor porus, an opening in the oculomotor triangle that forms the posterior part of the roof of the cavernous sinus and communicates with the basal cisterns. The trigonal segment of the oculomotor nerve is accompanied by the oculomotor cistern as it enters the superolateral cavernous sinus roof (Figs. 3C and 3D). This cistern has an average length of 6.5 mm (range, 3.0–11.0 mm). Its width is greatest at the oculomotor porus (average, 5.5 mm; range, 3.0–9.2 mm) and tapers slightly toward the midpoint of its length, where the average width is 4.4 mm (range, 3.0–7.1 mm). The diameters of the oculomotor nerve at the porus and the midpoint of the cisternal length average 2.7 mm (range, 1.5–4.1 mm) and 2.5 mm (range, 1.8–3.4 mm), respectively. At the oculomotor porus, the average distance between the nerve and the anterior border of the porus is 0.9 mm (range, 0–2.5 mm), and the distance between the nerve and the posterior edge of the cistern averages 2.2 mm (range, 0.8–3.7 mm) (Martins et al., 2006). The oculomotor porus has an elongated oval shape with its greatest diameter in the anteroposterior direction. The oculomotor nerve usually courses closer to the anterior than the posterior edge of the porus of the cistern (Figs. 3C and 4A). It occupies 48.3% of the total anteroposterior diameter of the cistern at the porus and is eccentrically located nearer its anterior than its posterior wall (Martins et al., 2006).

Figure 4. A: Lateral view of the right paraclinoid area. The cancellous bone of the ACP has been removed. The cortical portion of the ACP has been preserved to visualize the course of the oculomotor nerve. The cavernous segment of the oculomotor nerve is incorporated into the fibrous dural lateral wall of the cavernous sinus just under the tip of the ACP. B: The ACP has been removed to expose the carotid oculomotor membrane. The layer of dura that lines the lower margin of the ACP and extends medially to form the proximal dural ring is called the carotidoculomotor membrane. It separates the lower margin of the ACP from the cavernous segment of the oculomotor nerve and extends medially around the carotid artery. C: The optic canal has been unroofed and the anterior clinoid removed to expose the fissural segment of the oculomotor nerve. The greater wing of the sphenoid bone has been removed to expose the lateral rectus muscle, except for most medial part of the greater wing forming the lateral margin of the SOF. The oculomotor nerve splits into superior and inferior divisions 2–3 mm before its entrance into the SOF. D: The lateral margin of the SOF has been removed. The oculomotor, abducens, and nasociliary nerves enter the orbit through the annular tendon. The frontal, lacrimal, and trochlear nerves pass outside the annular tendon. Abbreviations: ACP., anterior clinoid process; Cavern., cavernous sinus; Clin., clinoid; CN., cranial nerve; Car. Oculo. Memb., carotidoculomotor membrane; Inf., inferior; Lac., lacrimal; Lat., lateral; Lev., levator; M., muscle; N., nerve; Nasocil., nasociliary; Rec., rectus; SOF., superior orbital fissure. (Images courtesy of AL Rhoton, Jr.)
The dural porus entry represents the main fixation point of the nerve (Figs. 3A and 3C). The other important fixation point is represented by the superior orbital fissure. These areas of attachment to the skull base could explain the high vulnerability of the nerve during pathological conditions (Iaconetta et al., 2010). An impression on the upper surface of the nerve is commonly observed at the level of the porus (Fig. 3C). The trigonal segment of the oculomotor nerve inside the oculomotor cistern is interposed between its free portion in the interpeduncular cistern and the part of its course where it is incorporated into the fibrous lateral wall of the cavernous sinus (Fig. 3D). This segment is well known to neurosurgeons as an avascular space used to expose and mobilize the nerve during cavernous sinus surgery (Fig. 3C) (Dolenc, 1983; Everton et al., 2008). The position of the oculomotor nerve nearer the anterior limit of the cistern at the oculomotor porus could make it more vulnerable to injury during approaches to the cavernous sinus that require opening the roof anterior to the nerve, as in the transcavernous approach to the basilar apex (Yasuda et al., 2005; Martins et al., 2006). Seoane et al. reasoned that opening the porus by incising the dura over an angled dissector introduced into the porus enhances the safety of this maneuver (Seoane et al., 2000).
CAVERNOUS SEGMENT
The cavernous sinuses are venous structures in the middle cranial base, surrounded by dural walls, which contain neurovascular structures and face the sella turcica, pituitary gland, and sphenoid bone on one side and the temporal lobe on the other (Renn and Rhoton, 1975). The trigonal segment of the oculomotor nerve passes through a short cistern in the roof of the cavernous sinus, the oculomotor cistern, and does not become incorporated into the lateral wall until it reaches the lower margin of the anterior clinoid process, where the cistern ends. The cavernous segment of the oculomotor nerve is finally incorporated into the fibrous dural lateral wall of the cavernous sinus just under the tip of the anterior clinoid process (Fig. 3D). This wall consists of two layers: the superficial dense layer formed by the dura mater, which faces the brain and contributes to creating the distal ring around the ICA, and a deep layer, which contributes to forming the proximal ring of the ICA from the endosteal layer between the oculomotor (III), trochlear (IV), and trigeminal (V1) nerves (Tuccar et al., 2000). The deep layer, an extension of the endosteal layer, invests the nerves running within the lateral wall of the cavernous sinus. The endosteal layer, at the level of the upper border of the maxillary nerve and the lower margin of the carotid sulcus, divides into two parts: one adheres to the sphenoid bone, covering the carotid sulcus and the floor of the sella, and other extends upward to constitute the internal layer of the lateral wall and roof of the cavernous sinus and diaphragm sellae (Figs. 3C and 3D) (Yasuda et al., 2004).
Dissections of the lateral sinus wall reveal that the thicker outer layer (a continuation of the dura mater) peels away, leaving the thin inner layer (a continuation of the endosteal layer) that invests the nerves in the lateral wall (Yasuda et al., 2005). Umansky reported that in 40% of their specimens the thinner, inner layer (an extension of the endosteal layer) was incomplete and often absent between cranial nerves III and V1, leaving a triangular opening on to the cavernous sinus cavity (Fig. 3D) (Umansky and Nathan, 1982). Kawase stated that the dural wall was very thin or missing between cranial nerves III and V1 and that tumor invasion could easily spread out from these openings (Kawase et al., 1996).
The layer of dura that lines the lower margin of the anterior clinoid process and extends medially to form the lower or proximal dural ring is called the carotidoculomotor membrane because it separates the lower margin of the anterior clinoid from the oculomotor nerve and extends medially around the carotid artery. Medially, this membrane also attaches the oculomotor nerve to the carotid (Figs. 4A and 4B). After piercing the cavernous sinus, the nerve reaches out of the lateral wall below the anterior clinoid process. It courses within the two dural layers of the lateral wall of the cavernous sinus, then along the lower edge of the anterior clinoid process to enter the superior orbital fissure. In the lateral wall of the cavernous sinus, it courses laterally and anteriorly to the dorsum sellae and above the meningohypophyseal trunk of the intracavernous segment of the ICA (Iaconetta et al., 2010). The length of the segment from the oculomotor porus to the point where the superior orbital fissure begins averages 15.4 mm on the right side and 14.9 mm on the left side, and its main diameter is 2.4 mm (Iaconetta et al., 2010).
FISSURAL SEGMENT
The superior orbital fissure is situated between the greater and lesser wings and the body of the sphenoid bone. It is roughly triangular, having a wide base medially on the sphenoid body and a narrow apex laterally between the lesser and greater wings. The fissure is not oriented in a strictly coronal plane but is directed forward so that the lateral apex is slightly forward of the medial margin. Its posterior margin is formed by the junction of the posterior margin of the optic strut with the anterior clinoid process (Figs. 4B and 4C). At the fissure, the dura covering the middle fossa and cavernous sinus blends into the periorbita of the orbital apex and the annular tendon from which the extraocular muscles arise. The annular tendon does not surround the whole superior orbital fissure but encompasses only the upper-medial portion, which is situated lateral to the optic strut and optic foramen (Figs. 4C and 4D).
The oculomotor nerve courses along the lateral surface of the optic strut as it passes through the medial part of the fissure. It splits into superior and inferior divisions 2–3 mm before its entrance into the superior orbital fissure (Fig. 4C) (Morard et al., 1994). The divisions pass through the oculomotor foramen on the medial side of the branches of the ophthalmic nerve. The oculomotor foramen, the central part of the superior orbital fissure, is bounded above by the annular tendon and the adjacent part of the lesser wing of the sphenoid bone, medially by the optic strut and the body of the sphenoid bone, laterally by the annular tendon and the prominence on the lateral margin of the fissure to which the annular tendon attaches, and below by the segment of the annular tendon spanning the interval between the body of the sphenoid and the bony prominence on the lateral edge of the fissure (Fig. 4C) (Natori and Rhoton, 1995). The abducens and nasociliary nerves and the branches of the carotid sympathetic plexus also pass through the oculomotor foramen. The oculomotor nerve is separated from the nasociliary nerve by the fibrous septum in this foramen. The optic nerve and ophthalmic artery pass through the optic foramen and the part of the annular tendon surrounding it (Fig. 5A).
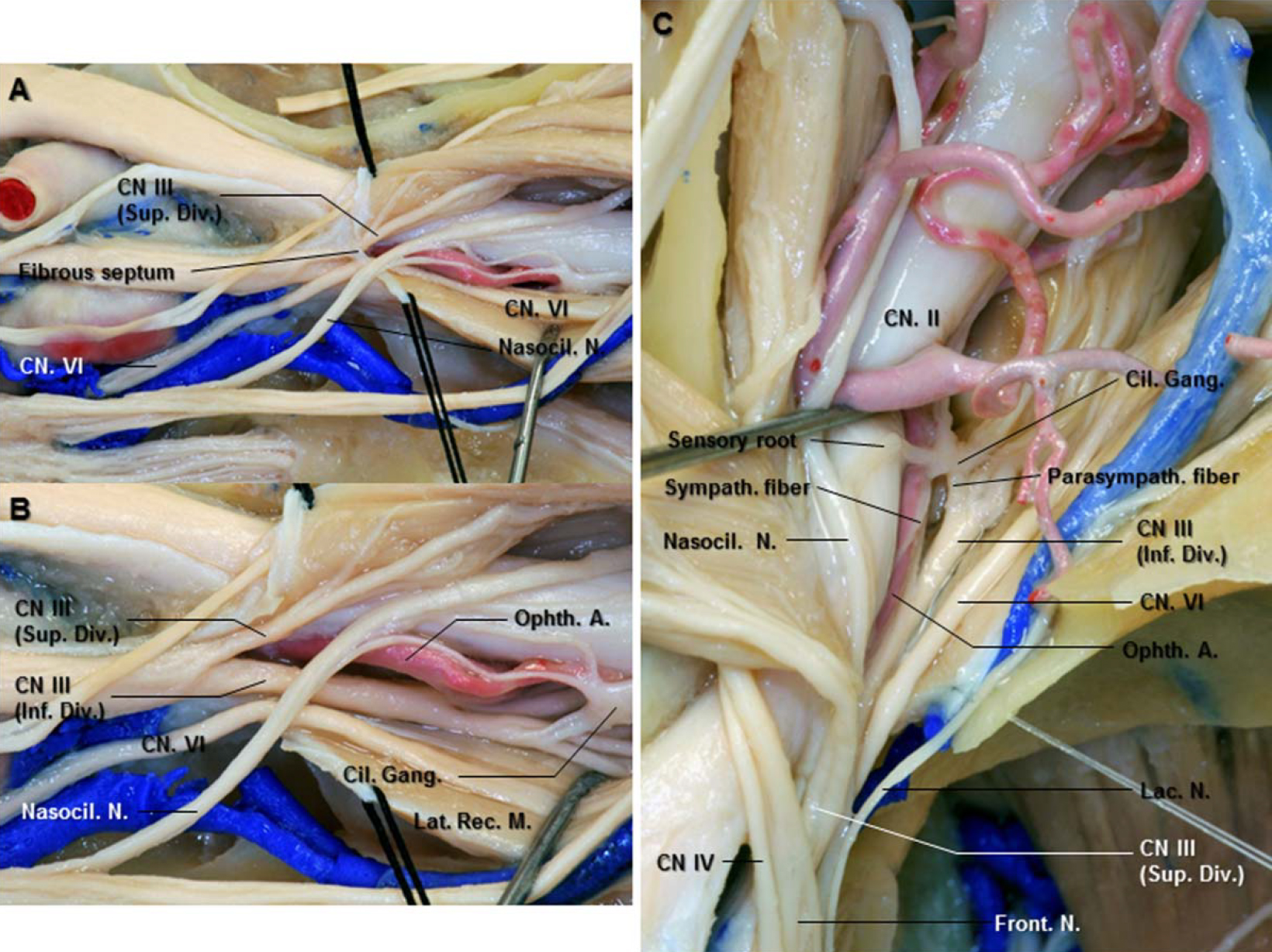
Figure 5. A: The annular tendon has been divided between the origin of the superior and lateral rectus muscles. The superior division of the oculomotor nerve passes upward to innervate the levator and superior rectus muscles. The inferior division courses inferior and medial as it proceeds through the SOF. The oculomotor nerve is separated from the nasociliary nerve by the fibrous septum in the oculomotor foramen. B: The fibrous septum has been removed to expose the oculomotor nerve in the foramen. At the orbital apex, the inferior division splits into three branches to innervate three muscles. The branch to the inferior oblique muscles gives rise to the motor parasympathetic root to the ciliary ganglion, situated on the inferolateral aspect of the optic nerve. C: The optic nerve has been retracted to the medial side to expose the sympathetic nerves that arise in the cervical sympathetic ganglia. The sensory root of the ciliary ganglion arises from the nasociliary nerve. Abbreviations: A., artery; Cil. Gang., ciliary ganglion; CN., cranial nerve; Div., division; Front., frontal; Inf., inferior; Lat., lateral; N., nerve; Nasocil., nasociliary; Ophth., ophthalmic; Parasympath., parasympathetic; Rec., rectus; Sup., superior; Sympath., sympathetic. (Images courtesy of AL Rhoton, Jr.)
The superior division courses below the lesser wing and enters the orbit below the origin of the superior rectus muscle from the annular tendon. It sends its branches upward into the lower margins of the levator and superior rectus muscles. It passes above the optic nerve to innervate the levator palpebrae and superior rectus muscles (Figs. 5A and 5B). The inferior division passes through the fissure on the medial side of the nasociliary and abducens nerves (Figs. 5B and 5C). At the orbital apex, it splits into branches to the inferior and medial rectus and inferior oblique muscles. The length of the fissural segment averages 6.9 mm on the right side and 5.9 mm on the left, and its main diameter is 2.5 mm (Iaconetta et al., 2010).
ORBITAL SEGMENT
The superior division of the oculomotor nerve enters the orbit through the superior orbital fissure superomedially to the nasociliary nerve just below the attachment of the superior rectus muscle to the annular tendon. It sends its branches upward lateral to the optic nerve to reach the lower surface of the superior rectus and levator muscles (Figs. 5B and 5C). Before ending on the inferior surface of the levator palpebrae superior muscle, this branch innervates the superior rectus muscle and then continues medially. A mean of five fibers (range, 3–7) innervate the superior rectus muscle, and a mean of one fiber (range, 1–2) follows a medial direction (84% of cases) or goes straight through the superior rectus muscle (16%); this single or double fiber divides into new fibers (mean of two; range, 1–5) and ends on the inferior surface of the levator palpebrae superior muscle (Zhang et al., 2010). The area embracing the oculomotor nerve from the medial side of the superior rectus muscle to the inferior surface of the levator palpebrae superior muscle is a key surgical landmark when the transcranial route to the orbit is taken (Iaconetta et al., 2010).
The inferior division courses inferiorly and medially as it proceeds through the superior orbital fissure on the medial side of the nasociliary and abducens nerves. At the orbital apex, it splits into three individual branches: two are directed forward to reach the inferior rectus and inferior oblique muscles, and one passes medially below the optic nerve to enter the medial rectus muscle (Figs. 5B and 5C and 6A). A mean of seven fibers (range, 3–10) innervate the inferior rectus muscle, the branch to which ends on the posterior one-third of the inferior rectus muscle in 84% of specimens and on the middle one-third in 16%. The longest branch runs forward between the inferior and lateral rectus muscles to innervate the inferior oblique muscle and contains a mean of five fibers (range, 3–7). The medial rectus muscle branch divides into a mean of six fibers (range, 3–8) (Zhang et al., 2010). The distance between the origin of the inferior division and the origin of the medial rectus muscle branch is 9.862.5 mm (range, 5.8–12.7 mm). In the orbit, the ophthalmic artery courses between the inferior and superior divisions, then reaches the inferolateral aspect of the optic nerve. It passes above the optic nerve in approximately 85% of orbits and below it in the remainder (Fig. 5C). When the ophthalmic artery passes above the optic nerve, it courses between the superior rectus muscle and the optic nerve and is adjacent to the superior division of the oculomotor nerve. If it passes below, it accompanies the medial rectus branches (Rhoton, 2002a; Zhang et al., 2010).
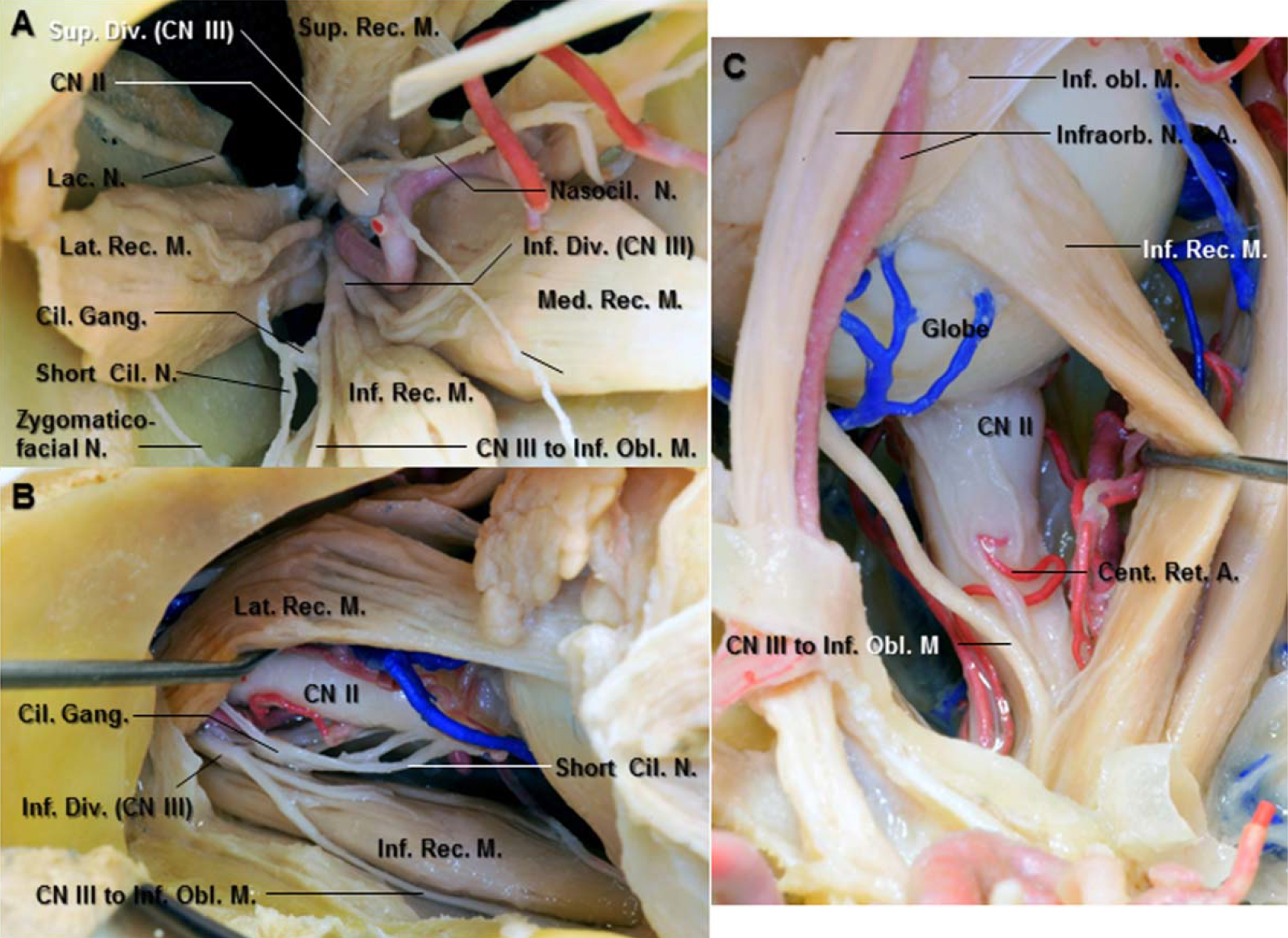
Figure 6. A: Anterior view of the right orbit after removal of the globe. Four rectus muscles are demonstrated. The inferior division splits into three branches. Two are directed to reach the inferior rectus and inferior oblique muscles, and one passes medially below the optic nerve to enter the medial rectus. B: Lateral view of the right orbit after removal of the lateral wall of the orbit. The lateral rectus muscle has been retracted superiorly to expose the ciliary ganglion and optic nerve. C: Inferior view of the right orbit after removal of the orbital floor. The inferior rectus muscle has been retracted medially to expose the optic nerve and the branch of the inferior division to the inferior oblique muscle. The central retinal artery pierces the lower surface of the optic nerve and courses a short distance inside the dural sheath of the nerve before passing to the center of the nerve, where it courses to the retina. Abbreviation: A., artery; Cent. Ret., central retinal; Cil. Gang., ciliary ganglion; CN., cranial nerve; Div., division; Inf., inferior; Infraorb., infraorbital; Lac., lacrimal; M., muscle; Med., medial; N., nerve; Obl., oblique; Rec., rectus. (Images courtesy of AL Rhoton, Jr.)
The branch to the inferior oblique muscle gives rise to the motor parasympathetic root to the ciliary ganglion, situated on the inferolateral aspect of the optic nerve and on the medial side of the lateral rectus muscle. The parasympathetic fibers synapse in the ciliary ganglion. Some of the ascending sympathetic fibers exit the carotid artery in the cavernous sinus and pass through the most medial part of the superior orbital fissure and oculomotor foramen to reach the ciliary ganglion and globe. The sympathetic fibers arise in the cervical sympathetic ganglia and pass through the ciliary ganglion without synapsing. The sensory root of the ciliary ganglion arises from the lower edge of the nasociliary nerve during passage through the lateral wall of the cavernous sinus or within the fissure (Figs. 5B and 5C and 6B) (Natori and Rhoton, 1995; Rhoton, 2002a). The ciliary ganglion is parasympathetic. It is situated in the back part of the orbit on loose fat between the optic nerve and the lateral rectus muscle, generally lying on the lateral side of the ophthalmic artery. The ganglion cells send a mean of seven (range, 4–11) short ciliary nerve fibers into the back of the eye, whence they ultimately innervate the ciliary muscle and the constrictor pupillae muscle (Figs. 5C and 6A and 6B) (Zhang et al., 2010).
CONCLUSIONS
The oculomotor nerve is a purely motor nerve that moves the eye, constricts the pupil, accommodates, and converges. It innervates four extraocular muscles and the levator palpebrae superior muscle, and consists of preganglionic parasympathetic fibers. It exits the brainstem from the interpeduncular fossa of the midbrain, passes through the lateral wall of the cavernous sinus, and enters the orbit via the superior orbital fissure. Knowledge of its detailed anatomy and pathway is critical for management of lesions at the level of the middle cranial fossa and in the clival, cavernous, and orbital regions.
Contributors: Hae Kwan Park, Hyung Keun Rha, Kyung Jin Lee, Chung Kee Chough, and Wonil Joo
Content from Park HK, Rha HK, Lee KJ, Chough CK, Joo W. Microsurgical anatomy of the oculomotor nerve. Clin Anat 2017;30:21–31. doi.org/10.1002/ca.22811.
The Neurosurgical Atlas is honored to maintain the legacy of Albert L. Rhoton, Jr, MD.
References
- Albayram S, Ozer H, Sarici A, Murphy K, Miller N. 2006. Unilateral mydriasis without ophthalmoplegia—A sign of neurovascular compression? Case report. Neurosurgery 58:E582–E583; discussion E582–E583.
- Anik I, Ceylan S, Koc K, Tugasaygi M, Sirin G, Gazioglu N, Sam B. 2011. Microsurgical and endoscopic anatomy of Liliequist’s membrane and the prepontine membranes: Cadaveric study and clinical implications. Acta Neurochir (Wien) 153:1701–1711.
- Atasever A, Durgun B, Celik HH, Yilmaz E. 1993. Somatotopic organization of the axons innervating the superior rectus muscle in the oculomotor nerve of the rat. Acta Anat (Basel) 146:251–254.
- Aygun D, Doganay Z, Baydin A, Akyol M, Senel A, Nural MS, Otal Y, Guven H. 2005. Posttraumatic pneumocephalus-induced bilateral oculomotor nerve palsy. Clin Neurol Neurosurg 108:84–86.
- Biller J, Shapiro R, Evans LS, Haag JR, Fine M. 1984. Oculomotor nuclear complex infarction. Clinical and radiological correlation. Arch Neurol 41:985–987.
- Brazis PW, Masdeu JC, Biller J. 2001. Ocular motor system. In: Localization in Clinical Neurology. 4th Ed. Philadelphia: Lippincott Williams & Wilkins. p 171–270.
- Buttner-Ennever JA. 2006. The extraocular motor nuclei: Organization and functional neuroanatomy. Prog Brain Res 151:95–125.
- Cano M, Lainez JM, Escudero J, Barcia C. 1989. Pituitary adenoma presenting as painful intermittent third nerve palsy. Headache 29:451–452.
- Caruso G, Vincentelli F, Rabehanta P, Giudicelli G, Grisoli F. 1991. Anomalies of the P1 segment of the posterior cerebral artery: Early bifurcation or duplication, fenestration, common trunk with the superior cerebellar artery. Acta Neurochir (Wien) 109:66–71.
- Castro O, Johnson LN, Mamourian AC. 1990. Isolated inferior oblique paresis from brain-stem infarction. Perspective on oculomotor fascicular organization in the ventral midbrain tegmentum. Arch Neurol 47:235–237.
- Clarke RJ, Coimbra CJ, Alessio ML. 1985. Distribution of parasympathetic motoneurones in the oculomotor complex innervating the ciliary ganglion in the marmoset (Callithrix jacchus). Acta Anat (Basel) 121:53–58.
- Dolenc V. 1983. Direct microsurgical repair of intracavernous vascular lesions. J Neurosurg 58:824–831.
- Dorland WAN. 2003. Dorland’s Illustrated Medical Dictionary. Philadelphia: Saunders.
- Everton KL, Rassner UA, Osborn AG, Harnsberger HR. 2008. The oculomotor cistern: Anatomy and high-resolution imaging. AJNR 29:1344–1348.
- Ford CS, Schwartze GM, Weaver RG, Troost BT. 1984. Monocular elevation paresis caused by an ipsilateral lesion. Neurology 34:1264–1267.
- Froelich SC, Abdel Aziz KM, Cohen PD, van Loveren HR, Keller JT. 2008. Microsurgical and endoscopic anatomy of Liliequist’s membrane: A complex and variable structure of the basal cisterns. Neurosurgery 63:ONS1–ONS8; discussion ONS8–ONS9.
- Goto K, Imai H, Nakazato O, Tsuda T, Okajima T. 1993. [Inferior branch palsy of the oculomotor nerve following clipping of basilar apex aneurysm]. Rinsho Shinkeigaku 33:203–206.
- Gould DJ, Fix JD. 2014. Neuroanatomy. Philadelphia: Lippincott Williams & Wilkins.
- Hall S, Carlin L, Roach ES, McLean WT. 1983. Pupillary sparing oculomotor palsy from metastatic carcinoma. Surg Neurol 19:363–364.
- Hashimoto M, Ohtsuka K, Akiba H, Harada K. 1998. Vascular compression of the oculomotor nerve disclosed by thin-slice magnetic resonance imaging. Am J Ophthalmol 125:881–882.
- Horn AK, Eberhorn A, Hartig W, Ardeleanu P, Messoudi A, Buttner-Ennever JA. 2008. Perioculomotor cell groups in monkey and man defined by their histochemical and functional properties: Reappraisal of the Edinger–Westphal nucleus. J Comp Neurol 507:1317–1335.
- Iaconetta G, de Notaris M, Cavallo LM, Benet A, Ensenat J, Samii M, Ferrer E, Prats-Galino A, Cappabianca P. 2010. The oculomotor nerve: Microanatomical and endoscopic study. Neurosurgery 66:593–601; discussion 601.
- Kawase T, van Loveren H, Keller JT, Tew JM. 1996. Meningeal architecture of the cavernous sinus: Clinical and surgical implications. Neurosurgery 39:527–534. discussion 534–526.
- Kozicz T, Bittencourt JC, May PJ, Reiner A, Gamlin PD, Palkovits M, Horn AK, Toledo CA, Ryabinin AE. 2011. The Edinger-Westphal nucleus: A historical, structural, and functional perspective on a dichotomous terminology. J Comp Neurol 519:1413–1434.
- Kraus MF, Little DM, Donnell AJ, Reilly JL, Simonian N, Sweeney JA. 2007. Oculomotor function in chronic traumatic brain injury. Cogn Behav Neurol 20:170–178.
- Ksiazek SM, Slamovits TL, Rosen CE, Burde RM, Parisi F. 1994. Fascicular arrangement in partial oculomotor paresis. Am J Ophthalmol 118:97–103.
- Liang C, Du Y, Lin X, Wu L, Wu D, Wang X. 2009. Anatomical features of the cisternal segment of the oculomotor nerve: Neurovascular relationships and abnormal compression on magnetic resonance imaging. J Neurosurg 111:1193–1200.
- Loewy AD, Saper CB, Yamodis ND. 1978. Re-evaluation of the efferent projections of the Edinger-Westphal nucleus in the cat. Brain Res 141:153–159.
- Madonick MJ, Ruskin AP. 1962. Recurrent oculomotor paresis. Paresis associated with a vascular anomaly, carotidbasilar anastomosis. Arch Neurol 6:353–357.
- Margolis TM, Newton TH, Hoyt WF. 1974. The posterior cerebral artery. Gross and roentgenographic anatomy. In: Newton TH, Potts DG, editors. Radiology of the Skull and Brain. Vol. 2. Saint Louis: Mosby. p 1551–1579.
- Mariak Z, Mariak Z, Stankiewicz A. 1997. Cranial nerve II-VII injuries in fatal closed head trauma. Eur J Ophthalmol 7:68–72.
- Martins C, Yasuda A, Campero A, Rhoton AL Jr. 2006. Microsurgical anatomy of the oculomotor cistern. Neurosurgery 58:ONS-220–ONS-227; discussion ONS-227–ONS-228.
- May PJ, Sun W, Erichsen JT. 2008. Defining the pupillary component of the perioculomotor preganglionic population within a unitary primate Edinger-Westphal nucleus. Prog Brain Res 171:97–106.
- Miyazaki S. 1985. Location of motoneurons in the oculomotor nucleus and the course of their axons in the oculomotor nerve. Brain Res 348:57–63.
- Morard M, Tcherekayev V, de Tribolet N. 1994. The superior orbital fissure: A microanatomical study. Neurosurgery 35:1087–1093.
- Mortazavi MM, Rizq F, Harmon O, Adeeb N, Gorjian M, Hose N, Modammadirad E, Taghavi P, Rocque BG, Tubbs RS. 2015. Anatomical variations and neurosurgical significance of Liliequist’s membrane. Childs Nerv Syst 31:15–28.
- Natori Y, Rhoton AL Jr. 1995. Microsurgical anatomy of the superior orbital fissure. Neurosurgery 36:762–775.
- Parent A, Carpenter MB. 1995. Carpenter’s Human Neuroanatomy. Baltimore: Williams & Wilkins.
- Porter JD, Baker RS. 1998. Anatomy and embryology of the oculomotor system. In: Miller NR, Newman NJ, Hoyt WF, Walsh FB, editors. Walsh and Hoyt’s Clinical Neuro-ophthalmology. 5th Ed. Baltimore; London: Williams & Wilkins. p 1055–1056.
- Purvin V. 2010. Photo essay. Isolated fascicular third nerve palsy. J Neuroophthalmol 30:263–265.
- Renn WH, Rhoton AL Jr. 1975. Microsurgical anatomy of the sellar region. J Neurosurg 43:288–298.
- Rhoton AL Jr. 2002a. The orbit. Neurosurgery 51:S303–S334. 3
- Rhoton AL Jr. 2002b. The supratentorial arteries. Neurosurgery 51:S53–S120.
- Saeki N, Murai H, Mine S, Yamaura A. 2000. Fascicular arrangement within the oculomotor nerve MRI analysis of a midbrain infarct. J Clin Neurosci 7:268–270.
- Seoane E, Tedeschi H, de Oliveira E, Wen HT, Rhoton AL Jr. 2000. The pretemporal transcavernous approach to the interpeduncular and prepontine cisterns: Microsurgical anatomy and technique application. Neurosurgery 46:891–898. Discussion 898–899.
- Srinivasan A, Dhandapani S, Kumar A. 2015. Pupil sparing oculomotor nerve paresis after anterior communicating artery aneurysm rupture: False localizing sign or acute microvascular ischemia? Surg Neurol Int 6:46.
- Sugimoto T, Itoh K, Mizuno N. 1978. Localization of neurons giving rise to the oculomotor parasympathetic outflow: A HRP study in cat. Neurosci Lett 7:301–305.
- Trobe JD. 1988. Third nerve palsy and the pupil. Footnotes to the rule. Arch Ophthalmol 106:601–602.
- Tuccar E, Uz A, Tekdemir I, Elhan A, Ersoy M, Deda H. 2000. Anatomical study of the lateral wall of the cavernous sinus, emphasizing dural construction and neural relations. Neurosurg Rev 23:45–48.
- Umansky F, Nathan H. 1982. The lateral wall of the cavernous sinus. With special reference to the nerves related to it. J Neurosurg 56:228–234.
- Uz A, Tekdemir I. 2006. Relationship between the posterior cerebral artery and the cisternal segment of the oculomotor nerve. J Clin Neurosci 13:1019–1022.
- Vitosevic Z, Marinkovic S, Cetkovic M, Stimec B, Todorovic V, Kanjuh V, Milisavljevic M. 2013. Intramesencephalic course of the oculomotor nerve fibers: Microanatomy and possible clinical significance. Anat Sci Int 88:70–82.
- Wang SS, Zheng HP, Zhang FH, Wang RM. 2011. Microsurgical anatomy of Liliequist’s membrane demonstrating three-dimensional configuration. Acta Neurochir (Wien) 153:191–200.
- Yasuda A, Campero A, Martins C, Rhoton AL Jr, Ribas GC. 2004. The medial wall of the cavernous sinus: Microsurgical anatomy. Neurosurgery 55:179–189. discussion 189–190.
- Yasuda A, Campero A, Martins C, Rhoton AL Jr, de Oliveira E, Ribas GC. 2005. Microsurgical anatomy and approaches to the cavernous sinus. Neurosurgery 56:4–27; discussion 24–27.
- Zhang Y, Liu H, Liu EZ, Lin YZ, Zhao SG, Jing GH. 2010. Microsurgical anatomy of the ocular motor nerves. Surg Radiol Anat 32:623–628.
Please login to post a comment.




