

Aspergillosis

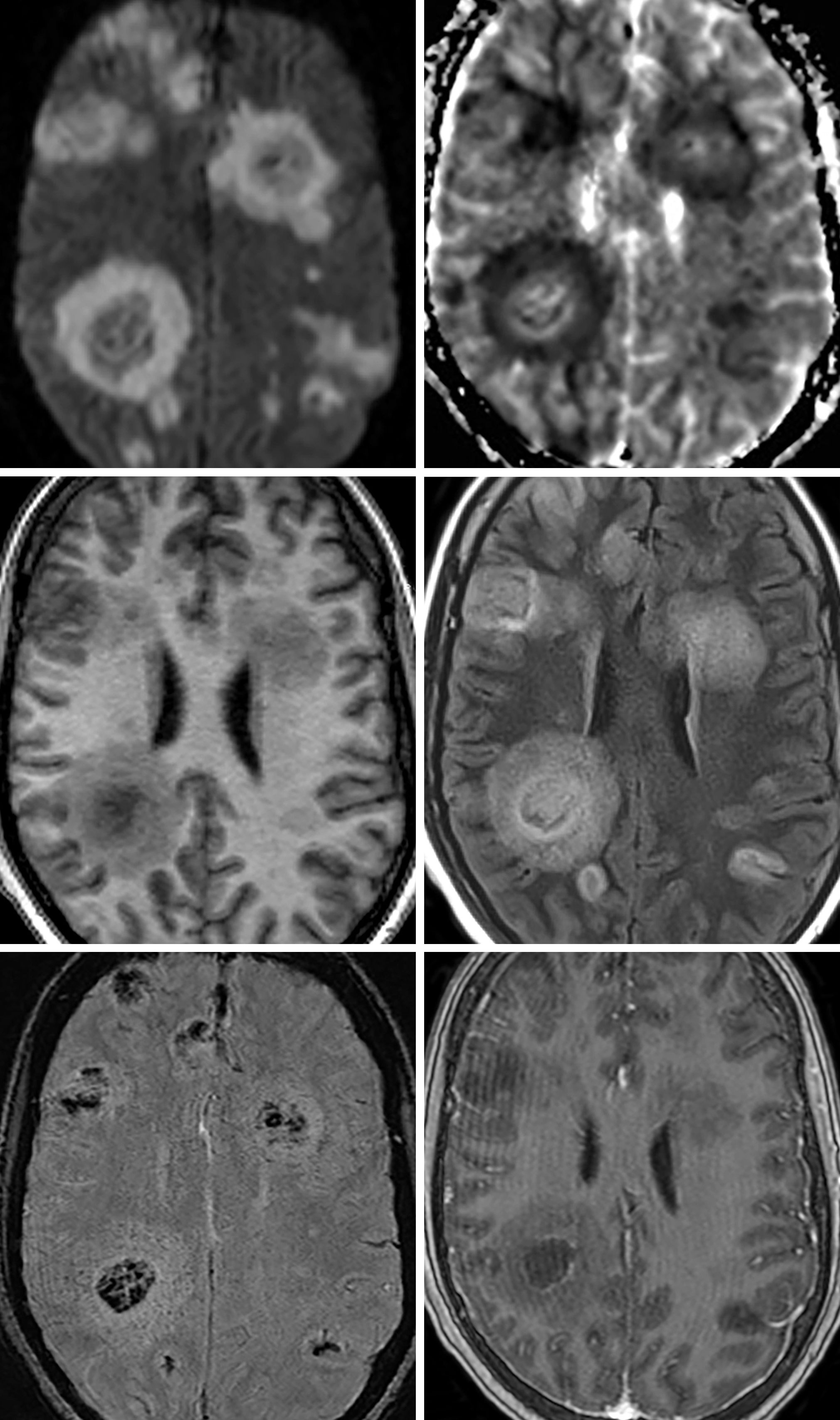
Figure 1: In this patient, there are multiple randomly distributed lesions scattered throughout bilateral cerebral hemispheres. (Top Left and Top Right) The lesions demonstrate a ring pattern, or rim of peripheral restricted diffusion and central hypointense DWI signal. (Middle Left and Middle Right) The rim pattern of signal abnormality carries through on all sequences. (Bottom Left) In this SWI image, there is central hypointense signal, which often corresponds to a combination of hemorrhage and fungal elements. (Bottom Right) As in most patients with aspergillosis, there is little to no peripheral enhancement.
Description
- Saprophytic opportunistic infection
Pathology
- Infection typically caused by Aspergillus fumigatus
- Septate, branching hyphae that show dichotomous branching and irregular, nonparallel cell walls
- Typically spreads hematogenously from the lungs
- Produce elastase, which leads to angioinvasion, microhemorrhage; mycotic aneurysm formation common, with resulting subarachnoid hemorrhage
- Fungal elements can also fill vessels, leading to occlusive thrombosis, embolism, and infarction
Clinical Features
- Symptoms
- Altered mental status, weakness, and seizures
- Population
- No age or gender predilection
- Underlying pulmonary illnesses are common
- Prognosis
- Poor, with mortality rate near 100%
Imaging
- General
- Multiple lesions with infarction or hemorrhage in a random distribution
- Predilection for perforating arteries—basal ganglia, thalamus, and corpus callosum
- Infarction of the corpus callosum is rare but suggests aspergillosis infection, because thromboembolism and pyogenic abscesses are uncommon in this location
- Meningitis and ventriculitis are common findings although often radiographically occult
- CT
- Not very specific
- Ill-defined hypodense regions with variable mass effect and vasogenic edema
- MRI
- T1WI
- Ill-defined hypointense foci
- T2WI
- Intermediate to low peripheral signal with central hyperintensity
- DWI
- Ring pattern—often hypointense centrally with peripheral diffusion restriction
- SWI
- Hypointense signal corresponding to focal hemorrhage and fungal elements
- Hemorrhage seen in 25% of patients
- Contrast
- None to weak peripheral
- T1WI
- Imaging recommendations
- Standard protocol MRI (including DWI) with intravenous contrast
- Mimic
- Given the wide variation in presentation (focal ring-enhancing lesion, meningeal involvement, infarctions, and hemorrhage), aspergillosis can be extremely difficult to diagnose accurately without the appropriate history; knowing the patient’s immune status can help narrow the differential substantially
For more information, please see the corresponding chapter in Radiopaedia.
Contributor: Sean Dodson, MD
References
Almutairi BM, Nguyen TB, Jansen GH, et al. Invasive aspergillosis of the brain: radiologic-pathologic correlation. Radiographics 2009;29:375–379. doi.org/10.1148/rg.292075143
DeLone DR, Goldstein RA, Petermann G, et al. Disseminated aspergillosis involving the brain: distribution and imaging characteristics. AJNR Am J Neuroradiol 1999;20:1597–1604.
Miszkiel KA, Hall-Craggs MA, Miller RF, et al. The spectrum of MRI findings in CNS cryptococcosis in AIDS. Clin Radiol 1996; 51(12):842–850. doi.org/10.1016/s0009-9260(96)80080-8
Rabelo NN, Silveira Filho LJ, da Silva BNB, et al. Differential diagnosis between neoplastic and non-neoplastic brain lesions in radiology. Arq Bras Neurocir 2016;35:45–61. doi.org/10.1055/s-0035-1570362
Starkey J, Moritani T, Kirby P. MRI of CNS fungal infections: review of aspergillosis to histoplasmosis and everything in between. Clin Neuroradiol 2014;24:217–230. doi.org/10.1007/s00062-014-0305-7
Tempkin AD, Sobonya RE, Seeger JF, et al. Cerebral aspergillosis: radiologic and pathologic findings. Radiographics 2006;26:1239–1242. doi.org/10.1148/rg.264055152
Please login to post a comment.




