

General Considerations



This is a preview. Check to see if you have access to the full video. Check access
Trigeminal neuralgia (TN) has been called one of the worst pains that can afflict a human being. John Fothergill was one of the first to describe this pain in his 1773 article: “On a Painful Affliction of the Face.” The pain of TN is relatively easy to diagnose—it is typically unilateral, episodic, severe, stabbing, shock-like or lancinating, and exacerbated by cutaneous stimuli such as tactile pressure, chewing, brushing, a breeze of air, or shaving. A crude annual incidence of TN is approximately 5.7 per 100,000 women and 2.5 per 100,000 men. Peak incidence lies between ages 50 and 60 years, and prevalence increases with age.
Initially a small dose of an antiepileptic drug (such as carbamazepine), rather than an analgesic drug, can provide excellent pain relief for TN. However, some patients do not respond to antiepileptic drugs or they suffer from adverse side effects, so they will qualify as candidates for one of the surgical procedures (microvascular decompression, stereotactic radiofrequency thermoablation, glycerol or balloon compression, and radiosurgery rhizotomy).
Regardless of the responsible etiology in the pathogenesis of this pain, MVD surgery, through mobilizing the offending vessel or by performing a rhizotomy, provides an effective and durable palliative option for symptomatic relief. Although percutaneous procedures offer a less invasive route to the Gasserian ganglion for rhizotomy, posterior fossa exploration is the only procedure that can identify an offending vessel via a nondestructive procedure with a more lasting result.
The patient’s age, medical comorbidities, and preferences are important factors that can limit the application of an MVD operation. I offer percutaneous procedures to my patients who are older than 70 years or who have prohibitive medical comorbidities that preclude their candidacy for an MVD operation. I also offer a percutaneous procedure to patients who have a diagnosis of multiple sclerosis and associated TN, regardless of their age.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features

Figure 1: One of the first patients of Harvey Cushing suffering from an attack of trigeminal neuralgia. This image is most likely one of the earliest photographs of a patient with this disease (Courtesy of Cushing Center at Yale University).
Pathogenesis
The pathogenesis of cranial nerve hyperactivity syndromes, such as TN, hemifacial spasm, geniculate neuralgia, paroxysmal positional vertigo, and glossopharyngeal neuralgia, has remained elusive. Vascular compression of the nerves near the brainstem (neurovascular conflict-peripheral hypothesis) has been proposed as the principal factor involved in genesis of cranial nerve hyperactivity through demyelination of the root entry/exit zone of the nerve (ephaptic transmission).
Recently, investigators have implicated other factors as causes for these disorders, including hyperactivity of the brainstem nuclei (central hypothesis).
Diagnosis and Evaluation
The diagnosis of TN and other episodic, unilateral neuralgiform pain disorders is based almost entirely on the patient’s history. The character of TN pain is typically unilateral and neuralgic: episodic, severe, stabbing, shock-like or lancinating, and exacerbated by cutaneous stimuli such as tactile pressure, chewing, brushing, a breeze of air, or shaving.
The periods of remission tend to get shorter over time and the attacks of pain often get longer. Patients may have as few as three or four attacks a day or as many as 70 per day. There is often a refractory period when the pain cannot be triggered. Pain can occur at night in a third of patients.
It is unusual to have TN in the first ophthalmic division of the trigeminal nerve only. The tentative desirable response to neuropathic pain medications, such as carbamazepine or gabapentin, often supports the diagnosis of typical TN. The pain characteristics may change with the use of neuropathic pain medications or previous percutaneous procedures, and may become more constant. Therefore, the clinician should inquire about the character of the pain at its inception before any treatment was rendered. Patients who complain of neuropathic pain (only constant or burning pain and facial numbness without triggering stimuli) are suffering from atypical facial pain, not TN, and are not candidates for the procedures described in the following chapters.
It is important to carefully examine the patient’s face and oral cavity along with the cranial nerves. Detailed neurologic examination of patients with TN is usually normal, but minor sensory changes in the corresponding distribution of the trigeminal nerve are fairly common. All patients who are planning to undergo any intervention for TN should have brain magnetic resonance imaging (MRI) or a computed tomography (CT) scan to exclude structural pathologies such as meningioma, acoustic neuroma, and epidermoid tumors. A vascular loop compressing the trigeminal nerve may be evident on high-resolution T2WI.
Indications for Percutaneous Treatment of Trigeminal Neuralgia
Treatment of all patients with classical TN begins with drug therapy, usually anticonvulsants, and the gold standard is carbamazepine. Newer drugs such as oxcarbazepine are rapidly gaining popularity due to better side-effect profiles. These medications can initially provide 100% pain relief in 70% of patients. However, despite the use of neuropathic pain medications, many patients’ pain becomes refractory and they seek more durable surgical treatment.
Indications for surgical intervention include, but are not limited to, failure of or adverse side effects from medical treatment. Microvascular decompression (MVD) has been shown to provide the most durable satisfactory results; however, patients older than 70 years or with associated prohibitive medical morbidities or conditions that preclude general anesthesia can be considered suitable candidates for less invasive percutaneous or radiosurgical procedures.
Percutaneous procedures for TN are palliative destructive procedures that involve controlled damage to the trigeminal nerve root with the goal of relieving pain. These procedures include radiofrequency rhizotomy/thermoablation, glycerol rhizotomy, and balloon compression. All of these procedures are performed via a foramen ovale puncture, which was first described by Härtel in 1914. We will discuss these modalities individually and their advantages and potential pitfalls.
Treatment Paradigm
For patients who cannot undergo an MVD operation, I generally prefer balloon compression rhizotomy because it is easy to perform and immediately effective. Radiosurgery often does not offer immediate pain relief and many patients continue to require neuralgic medications for their pain control.
If the patient harbors comorbidities that preclude the use of general anesthesia and immediate pain relief is not a concern, I offer radiosurgery as a reasonable option.
I use the algorithmic approach shown in the following illustration for selection of the operative intervention.

Preoperative Considerations
Patients who are candidates for percutaneous treatment of TN are generally elderly and harbor multiple medical comorbidities. These patients should undergo extensive preoperative anesthesia evaluation to assess their cardiac and respiratory status. Special emphasis should be placed on cardiac evaluation since a high proportion of patients will experience bradycardia and hypotension secondary to trigeminal depressor response once the foramen ovale is accessed. For this reason, some surgeons advocate placing a transcutaneous or a transesophageal pacemaker after induction of anesthesia.
Patients should be encouraged to learn how to localize and designate where they perceive facial stimulation during radiofrequency ablation. Patients are encouraged to discontinue anticoagulation 5-7 days before the procedure, although this is not absolutely necessary. A baseline neurologic exam focusing on the face should be performed. Corneal reflex and any areas of facial numbness are carefully documented. Furthermore, weakness in any of the trigeminal innervated muscles (masseter, pterygoids) should also be noted. Dentures should be removed before the procedure. Preoperative neuropathic pain medications should be continued and tapered off gradually in the postoperative period.
Patients who suffer from numbness in the distribution of their pain are not candidates for percutaneous procedures.
Procedures: Please refer to the following individual chapters regarding the specifics of technique:
Postoperative Considerations
After any percutaneous procedure, I prefer to keep patients under observation for 2 to 4 hours before their discharge. An immediate postoperative examination should examine facial and corneal sensation and motor strength of the masseter, pterygoids, ocular, and facial muscles. Any bleeding from the needle insertion site can be simply treated by applying pressure. Meticulous eye care is needed in cases when corneal reflex is likely to be compromised.
Preoperative medications are continued and slowly tapered over the next 2 weeks. Patients and their family members should be given basic instructions about numbness in the face and eyes. They should be informed about the small likelihood of cold sores a few days after the procedure and instructed to contact their treating physicians. Fever and confusion during the 2-week postoperative period should raise the suspicion of meningitis.
Complications
Multiple structures surround the trigeminal ganglion, including the carotid artery, cranial nerves along and within the cavernous sinus, and the temporal lobe. All these structures are at risk if the selected trajectory is erroneous. The percutaneous procedures also place the cardiovascular system under stress, so our anesthesiologist colleagues should consider relevant risks.
Potential complications include:
- Penetration of the Buccal Mucosa: Care should be taken not to violate the buccal mucosa while guiding the needle/cannula toward the foramen ovale. An unnoticed buccal mucosal violation increases the likelihood of postoperative bacterial meningitis. I use my index finger to palpate and guide the tip of the cannula to ensure mucosal integrity.
If inadvertent violation of the mucosa occurs, the needle/cannula should be exchanged for a new one and a different submucosal tract used to enter the foramen. -
Injury to the Internal Carotid Artery: The internal carotid artery and other vascular structures can be injured by the needle in three locations while approaching the foramen: 1) The C2 segments as the needle tip enters the petrous bone too posteriorly, 2) The C3 segment if the needle is directed too posterolaterally, and 3) The C4 segment if the needle is navigated too anteromedially.
If pulsatile arterial blood is seen ejecting from the needle, the needle should be removed and manual pressure applied at the posterior pharyngeal space. The procedure should be aborted and a CT angiogram performed to exclude the presence of an arterial wall dissection or pseudoaneurysm formation.
- Injury to the Cranial Nerves and Temporal Lobe: An angulated anterosuperior trajectory to the foramen can direct the needle to enter the inferior orbital fissure and contact the V2 division. Moreover, deep penetration of the needle beyond the clival line can injure cranial nerves (CN’s) IV and VI. A far lateral trajectory can place the needle within the subdural space and injure the temporal lobe. Blindness may also occur from excessive cranial angulation with penetration of the inferior orbital fissure and by directly traumatizing the optic nerve within the orbital apex.
- Cardiovascular Stress: When the foramen ovale is engaged with a needle or cannula, a trigeminal depressor response occurs in about 20% or more of patients. This response leads to bradycardia and hypotension or to hypertension and tachycardia. These abrupt cardiovascular changes also occur when the balloon is inflated during balloon compression or when glycerol is injected during a glycerol rhizotomy. If the team is not prepared, occasionally a patient may suffer cardiac arrest. To address this risk, premedication with atropine or placement of a transcutaneous pacemaker is recommended. Some operators advocate administration of local anesthetic in the vicinity of the foramen to blunt the cardiovascular response.
- Sensory Disturbances: Postoperative trigeminal sensory numbness is quite common after radiofrequency and balloon compression rhizotomy and less common after glycerol rhizotomy. It is considered more of a side effect than a complication. However, corneal numbness and subsequent keratitis may be more common after radiofrequency and glycerol rhizotomy (10%), and its risk is considered negligible after balloon compression. Anesthesia dolorosa or severe deafferentation pain can be seen in up to 5 to 10% of patients after any ablative treatment modality and is very difficult to treat. Therefore, although mild sensory loss is desirable, significant nerve injury leading to severe numbness must be avoided.
- Motor Weakness: Masseter muscle weakness occurs postoperatively in virtually all patients undergoing balloon compression and in a minority of patients after radiofrequency rhizotomy. Masseter weakness is mostly transient and resolves in a few weeks. However, more than 10% of patients may experience long-term mastication difficulties.
- Herpes Labialis: Herpes simplex labialis has a tendency to exacerbate after any percutaneous trigeminal procedure, and although this is common, it is usually transient. Vesicular eruptions appear 3 to 4 days after the procedure and remit spontaneously. Some surgeons advocate using acyclovir prophylactically.
According to a systematic review of ablative neurosurgical techniques for treatment of TN (Lopez et al., 2004), radiofrequency rhizotomy is associated with the greatest number of cumulative complications (29.2%), followed by glycerol rhizotomy (24.8%), and balloon compression (16.1%). However, the risk of vascular and nerve injuries and meningitis was highest with balloon compression. Permanent facial sensory loss is most common after radiofrequency rhizotomy and can affect the quality of life in up to two-thirds of patients (Zakrzewska et al., 1999).
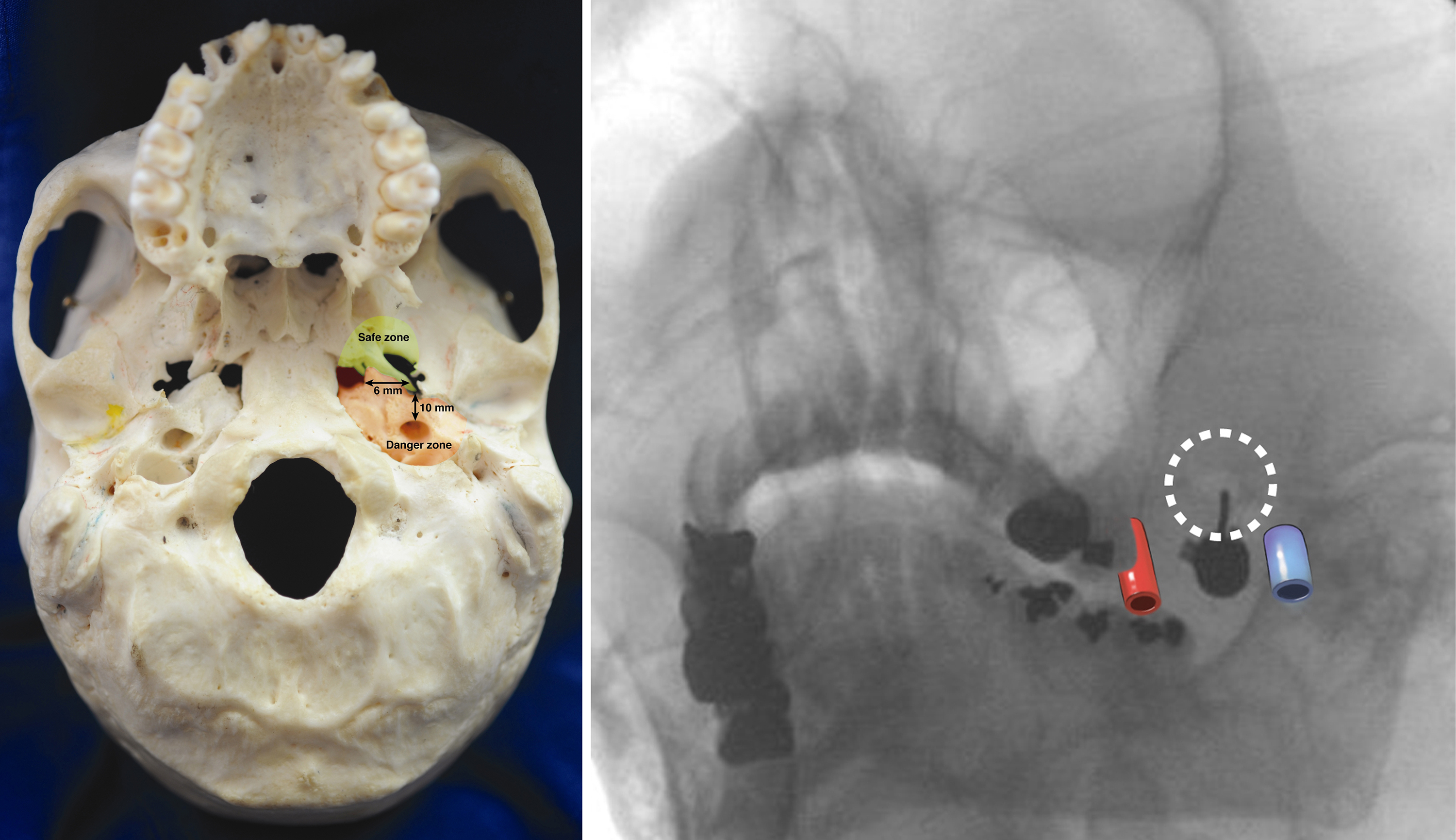
Figure 2: The safe (green) and danger (orange) zones for navigating the trajectory of the needle (left image). The approximate locations of the left internal carotid artery and jugular vein are demonstrated on an oblique intraoperative X-ray obtained parallel to the needle (right image).
Pain Control and Recurrence Rates
Radiofrequency Rhizotomy: Initial pain relief rates as high as 97.6% were reported in a study of 1,600 patients, with complete pain relief rates of 92% at 60 months and 97% at 180 months when patients were treated multiple times (Kanpolat et al., 2001). According to a systematic review (Lopez et al., 2004), radiofrequency rhizotomy seems to provide the highest rates of sustained complete pain relief among percutaneous techniques.
Recurrence rates ranging from 7.8% to 25% at 11.6 and 14 years, respectively, were reported by two studies (Fraioli et al., 2009, and Taha et al., 1995). Tronnier et al. reported a 50% rate of pain recurrence after 2 years and 75% after 4.5 years in patients who underwent radiofrequency rhizotomy (Tronnier et al., 2001). Overall, radiofrequency rhizotomy lesioning generally provides a longer duration of pain freedom and lower recurrence rate than either balloon compression (Taha et al., 1996) or glycerol rhizotomy (Lopez et al., 2004).
Glycerol Rhizotomy: A recent study of 3,370 patients revealed initial pain relief of >90%, with pain recurring in 35% over a period of 23 years, whereas most (21%) of these recurrences occurred within 5 years of the initial procedure (Xu-Hui et al., 2011). Other reports mention complete pain relief at 6 months and 3 years ranging from 78% to 88% and 53% to 54%, respectively (Slettebo et al., 1993, and North et al., 1990).
According to Pollock (2005), the only statistically significant predictor of positive treatment outcome was pain during glycerol injection. The therapeutic effects of glycerol decreased rapidly after 24 months, and glycerol rhizotomy seemed to be the least beneficial of the three techniques at 36 months (Lopez et al., 2004). According to Tatli et al. (2008), the recurrence rate was highest after glycerol rhizotomy (62%).
Balloon Compression: Balloon compression offers excellent initial pain relief, with rates as high as 94% in a study of 50 patients (Brown et al., 1993). Actuarial rates of complete pain relief were 91% and 69% at 6 months and 3 years, respectively. More recently, Asplund et al. (2010) reported results from 87 procedures with an initial success rate of 94% and a median pain-free time of 28 months. Recurrence rates were high (average, 26% with a mean time to recurrence of 18 months; Brown et al., 1993).
Although the procedure can be repeated, the results of a new compression are perhaps not likely to last as long (Fraioli et al., 1989), and the subsequent success rates may be lower (Kouzounias et al., 2010).
Pearls and Pitfalls
- Trigeminal neuralgia is characterized by paroxysmal attacks of unilateral, sharp, stabbing facial pain within one or more divisions of the trigeminal nerve, lasting <1 second to 2 minutes and precipitated by stimulation of certain trigger zones.
- Medical treatment with carbamazepine should be the first line of treatment in patients with TN. Patients with TN refractory to medications are candidates for MVD surgery or other ablative procedures.
- Although MVD yields the most satisfactory results, patients older than 70 years or with associated prohibitive medical morbidities that preclude a craniotomy or lengthy anesthesia should be considered for less invasive, percutaneous ablative procedures such as radiofrequency, glycerol, or balloon compression rhizotomy.
- Safe and efficient access to the foramen ovale is key to delivering an effective percutaneous treatment. The foramen ovale can be accessed using Hartel’s anatomic landmarks. The surgeon should be aware of the neighboring neurovascular structures to avoid complications.
- Radiofrequency rhizotomy has the advantage of mapping the nerve before lesioning, but requires an awake and cooperative patient. Radiofrequency rhizotomy generally offers a longer duration of pain relief and lower recurrence rate than other techniques, but may carry a higher complication rate.
- Glycerol rhizotomy offers excellent initial pain relief, but its effects wane over time and it has the highest recurrence rate.
- Balloon compression is ideal for candidates with isolated V1-distribution TN since it spares the corneal reflex.
References
Agazzi S, Chang S, Drucker MD, Youssef AS, Van Loveren HR. Sudden blindness as a complication of percutaneous trigeminal procedures: Mechanism analysis and prevention. J Neurosurg. 2009;110:638-641.
Arrese I, Lobato RD, Alén JF, Lagares A, Miranda P. Acute subdural and intratemporal hematoma as a complication of percutaneous compression of the gasserian ganglion for trigeminal neuralgia. Neurocirugia (Astur). 2005;16:177-182.
Asplund P, Linderoth B, Bergenheim AT. The predictive power of balloon shape and change of sensory functions on outcome of percutaneous balloon compression for trigeminal neuralgia. J Neurosurg. 2010;113:498-507.
Bergenheim AT, Asplund P, Linderoth B. Percutaneous retrogasserian balloon compression for trigeminal neuralgia: Review of critical technical details and outcomes. World Neurosurg. 2013;79:359-368.
Brown JA, McDaniel MD, Weaver MT. Percutaneous trigeminal nerve compression for treatment of trigeminal neuralgia: Results in 50 patients. Neurosurgery. 1993;32:570-573.
Cheng JS, Lim DA, Chang EF, Barbaro NM. A review of percutaneous treatments for trigeminal neuralgia. Neurosurgery. 2014;Suppl 1:25-33
de Siqueira SR, da Nobrega JC, de Siqueira JT, Teixeira MJ. Frequency of postoperative complications after balloon compression for idiopathic trigeminal neuralgia: Prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:e39-e45.
Fraioli MF, Cristino B, Moschettoni L, Cacciotti G, Fraioli C. Validity of percutaneous controlled radiofrequency thermocoagulation in the treatment of isolated third division trigeminal neuralgia. Surg Neurol. 2009;71:180-183.
Fraioli B, Esposito V, Guidetti B, Cruccu G, Manfredi M. Treatment of trigeminal neuralgia by thermocoagulation, glycerolization, and percutaneous compression of the gasserian ganglion and/or retrogasserian rootlets: Long-term results and therapeutic protocol. Neurosurgery. 1989;24:239-245.
Kanpolat Y, Savas A, Bekar A, Berk C. Percutaneous controlled radiofrequency trigeminal rhizotomy for the treatment of idiopathic trigeminal neuralgia: 25-year experience with 1,600 patients. Neurosurgery. 2001;48:524-532.
Kondziolka D, Lunsford LD. Percutaneous retrogasserian glycerol rhizotomy for trigeminal neuralgia: Technique and expectations. Neurosurg Focus. 2005;18:E7.
Kouzounias K, Schechtmann G, Lind G, Winter J, Linderoth B. Factors that influence outcome of percutaneous balloon compression in the treatment of trigeminal neuralgia. Neurosurgery. 2010;67:925-934.
Lobato RD, Rivas JJ, Sarabia R, Lamas E. Percutaneous microcompression of the gasserian ganglion for trigeminal neuralgia. J Neurosurg. 1990;72:546–553.
Lopez BC, Hamlyn PJ, Zakrzewska JM. Systematic review of ablative neurosurgical techniques for the treatment of trigeminal neuralgia. Neurosurgery. 2004;54:973-982.
Matsuda S, Serizawa T, Sato M, Ono J. Gamma knife radiosurgery for trigeminal neuralgia: The dry-eye complication. J Neurosurg. 2002;97:525–528.
North RB, Kidd DH, Piantadosi S, Carson BS. Percutaneous retrogasserian glycerol rhizotomy: Predictors of success and failure in treatment of trigeminal neuralgia. J Neurosurg. 1990;72:851-856.
Peris-Celda M, Graziano F, Russo V, Mericle RA, Ulm AJ. Foramen ovale puncture, lesioning accuracy, and avoiding complications: Microsurgical anatomy study with clinical implications. J Neurosurg. 2013;119:1176-1193.
Pollock BE. Percutaneous retrogasserian glycerol rhizotomy for patients with idiopathic trigeminal neuralgia: A prospective analysis of factors related to pain relief. J Neurosurg. 2005;102:223-228.
Rhoton AL Jr. The anterior and middle cranial base. Neurosurgery. 2002(Sup 1);51:273-302.
Slettebo H, Hirschberg H, Lindegaard KF. Long-term results after percutaneous retrogasserian glycerol rhizotomy in patients with trigeminal neuralgia. Acta Neurochir (Wien). 1993;122:231-235.
Taha JM, Tew JM Jr. Comparison of surgical treatments for trigeminal neuralgia: Reevaluation of radiofrequency rhizotomy. Neurosurgery. 1996;38:865-871.
Taha JM, Tew JM Jr, Buncher CR. A prospective 15-year follow up of 154 consecutive patients with trigeminal neuralgia treated by percutaneous stereotactic radiofrequency thermal rhizotomy. J Neurosurg. 1995;83:989-993.
Tatli M, Satici O, Kanpolat Y, Sindou M. Various surgical modalities for trigeminal neuralgia: Literature study of respective long-term outcomes. Acta Neurochir (Wien). 2008;150:243-255.
Tew JM, Grande A. Percutaneous stereotactic radiofrequency treatment of trigeminal neuralgia. COSMAN Procedure Technique Series. Available at: http://www.mayfieldclinic.com/trigeminal/COSMAN_PSR_technique_series.pdf
Tronnier VM, Rasche D, Hamer J, Kienle AL, Kunze S. Treatment of idiopathic trigeminal neuralgia: Comparison of longterm outcome after radiofrequency rhizotomy and microvascular decompression. Neurosurgery. 2001;48:1261–1267.
Xu-Hui W, Chun Z, Guang-Jian S, Min-Hui X, Guang-Xin C, Yong-Wen Z, Lun-Shan X. Long-term outcomes of percutaneous retrogasserian glycerol rhizotomy in 3370 patients with trigeminal neuralgia. Turk Neurosurg. 2011;21:48-52.
Zakrzewska JM, Jassim S, Bulman JS. A prospective, longitudinal study on patients with trigeminal neuralgia who underwent radiofrequency thermocoagulation of the gasserian ganglion. Pain. 1999;79:51–58.
Please login to post a comment.




