

Intracranial Lipoma

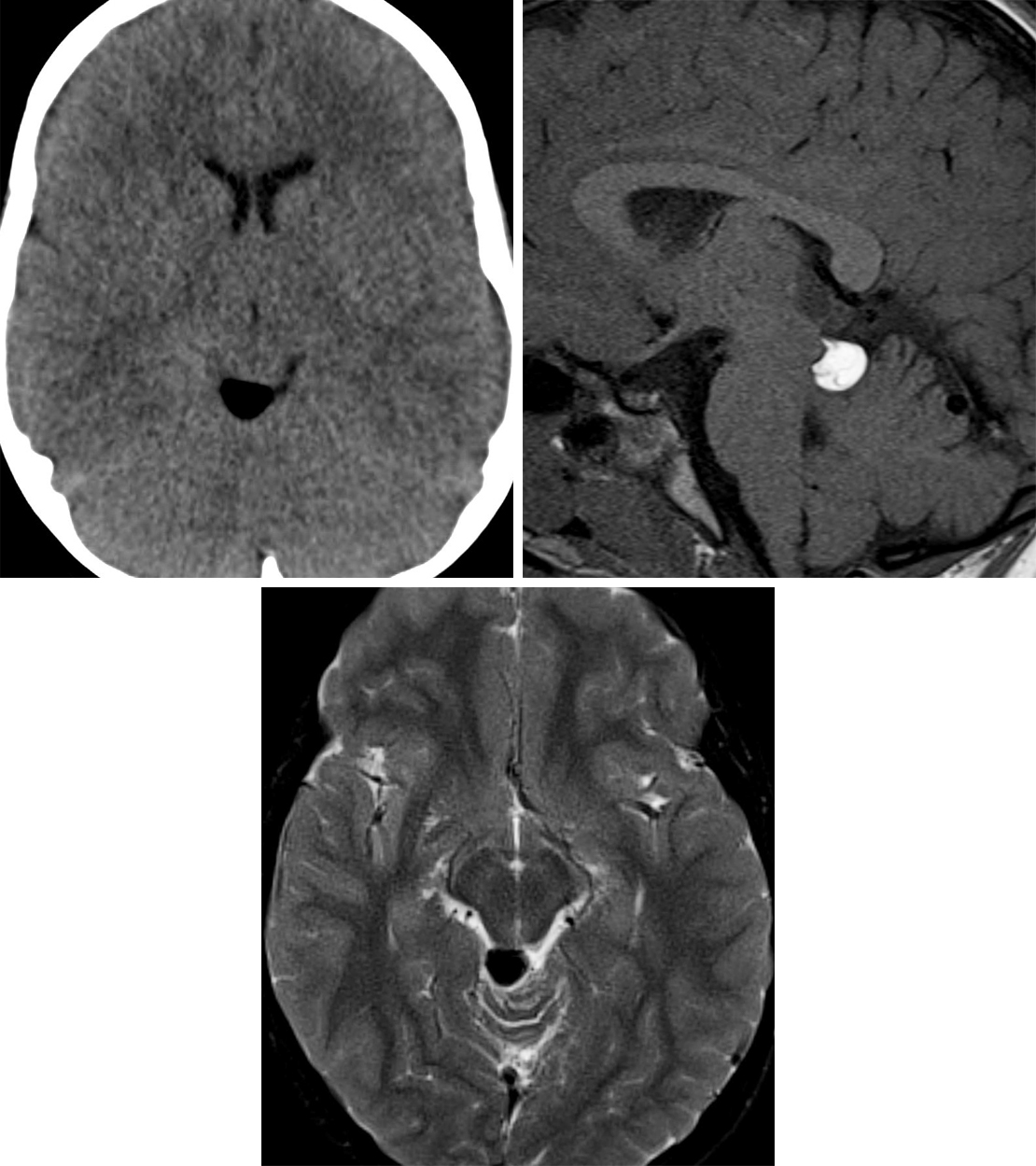
Figure 1: This tectal plate lipoma demonstrates low density of fat on CT imaging (top left) and hyperintensity on T1WI (top right). (Bottom) Fat-suppression techniques should make the lesion appear dark, as on this axial T2-weighted fat-saturated sequence.

Figure 2: Axial (top left) and sagittal (top right) T1-weighted images demonstrate an intrinsically T1 hyperintense pericallosal mass that is suppressed on T2-weighted fat-saturation imaging (bottom). The appearance and location are classic for intracranial lipoma, resulting from a developmental failure of the meninx primitiva to involute.
BASIC DESCRIPTION
- Fat-containing developmental or congenital abnormalities of neural crest origin
- Rarely neoplastic

ATLAS Choice Bipolar Forceps
Designed for your every surgical maneuver
Five tip sizes for brain and spine procedures
Unparalleled non-stick and low-profile features
PATHOLOGY
- Arise secondary to abnormal differentiation of the meninx primitiva
- Associated with other neural crest congenital anomalies in 60% of cases, often agenesis of the corpus callosum or underdevelopment of the inferior colliculus
- Located in the pericallosal region or within the quadrigeminal, suprasellar, or cerebellopontine angle cisterns
CLINICAL FEATURES
- All ages affected
- Common presenting signs/symptoms
- Usually asymptomatic (incidental finding on imaging performed for other reasons)
- Treatment: usually no treatment required; resection or cerebrospinal fluid shunting if large with mass effect or hydrocephalus
IMAGING FEATURES
- General
- Well-marginated, low-attenuation or high-signal-intensity mass (fat density)
- CT
- Hypoattenuating (–20 to –100 Hounsfield units)
- ±Peripheral calcification
- No enhancement on contrast-enhanced CT imaging
- MRI
- T1WI: hyperintense
- T2WI: similar signal as scalp fat
- Suppresses on fat-saturated sequences
- T1WI+C: no enhancement
IMAGING RECOMMENDATIONS
- CT imaging is often definitive, MRI without and with intravenous contrast might be necessary to exclude mimics
For more information, please see the corresponding chapter in Radiopaedia.
Contributors: Rachel Seltman, MD, and Jacob A. Eitel, MD
References
Gossner J. Small intracranial lipomas may be a frequent finding on computed tomography of the brain. A case series. Neuroradiol J 2013;26:27–29. doi.org/10.1177/197140091302600104.
Jabot G, Stoquart-Elsankari S, Saliou G, et al. Intracranial lipomas: clinical appearances on neuroimaging and clinical significance. J Neurol 2009;256:851–855. doi.org/10.1007/s00415-009-5087-5.
Osborn AG, Salzman KL, Jhaveri MD. Diagnostic Imaging (3rd ed). Elsevier, Philadelphia, PA; 2016.
Yildiz H, Hakyemez B, Koroglu M, et al. Intracranial lipomas: importance of localization. Neuroradiology 2006;48:1–7. doi.org/10.1007/s00234-005-0001-z.
Please login to post a comment.




