

Arachnoid Cyst (AC)


Figure 1: (Top Left and Right) This left middle crania fossa extra-axial lesion follows CSF on all sequences and is in a very common location for arachnoid cyst. Note how the temporal lobe is displaced but is without edema. (Bottom) No diffusion restriction is present that would suggest this lesion to be an epidermoid cyst. Given the degree of mass effect, for most other lesions one would expect evidence of cerebral herniation, a finding not typically seen with arachnoid cysts.
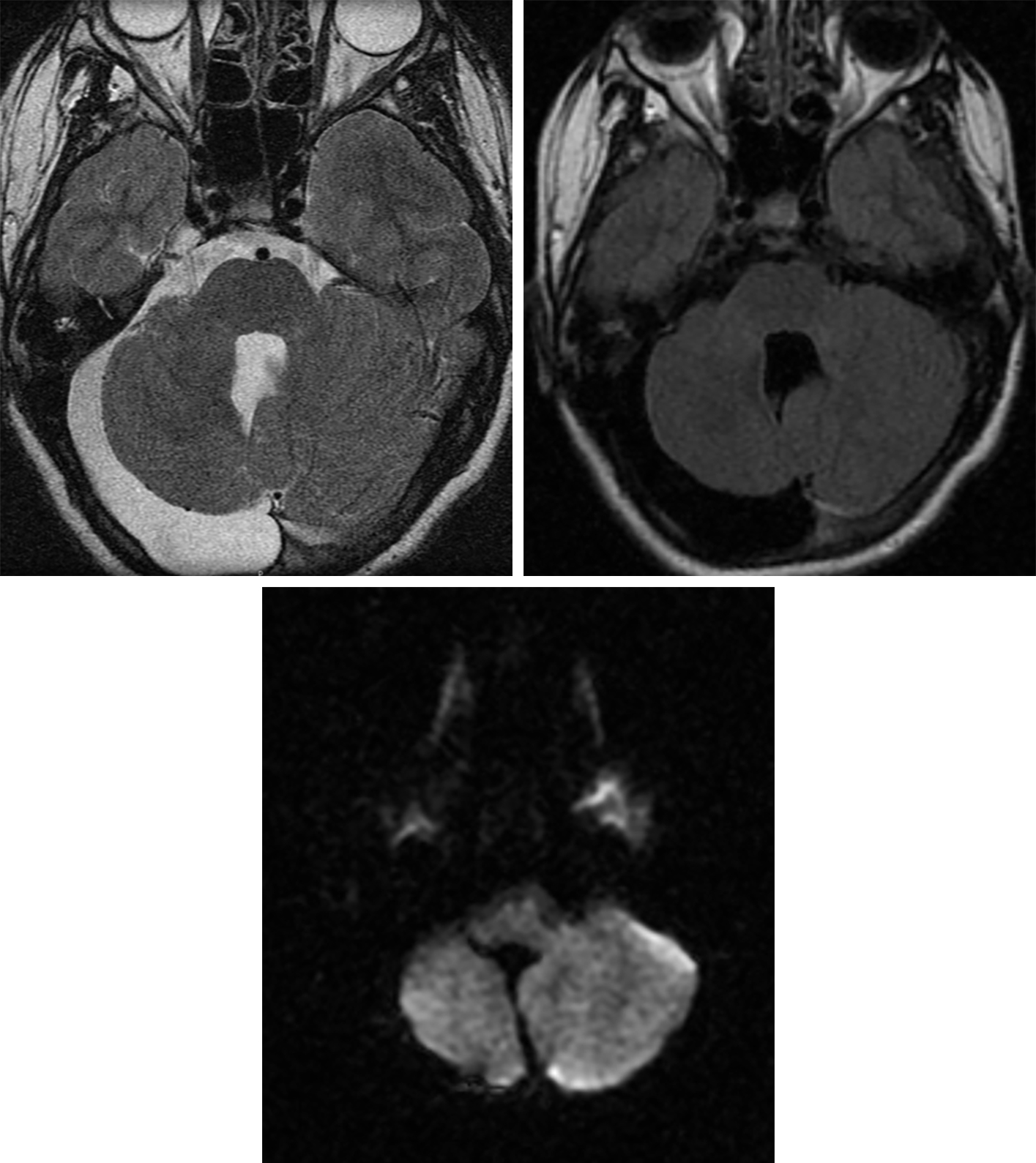
Figure 2: This arachnoid cyst posterior to the right cerebellar hemisphere demonstrates T2 hyperintensity (top left) and completely suppresses on FLAIR (top right), matching the CSF in the fourth ventricle on both of these sequences. It exhibits no DWI hyperintensity (bottom), distinguishing this arachnoid cyst from an epidermoid cyst. The mass effect on the adjacent cerebellum is somewhat substantial, but the parenchyma is without edema, suggesting a chronic or developmental abnormality. The calvarium is also thinned overlying the cyst on T2 (top left), another characteristic that implies chronicity.
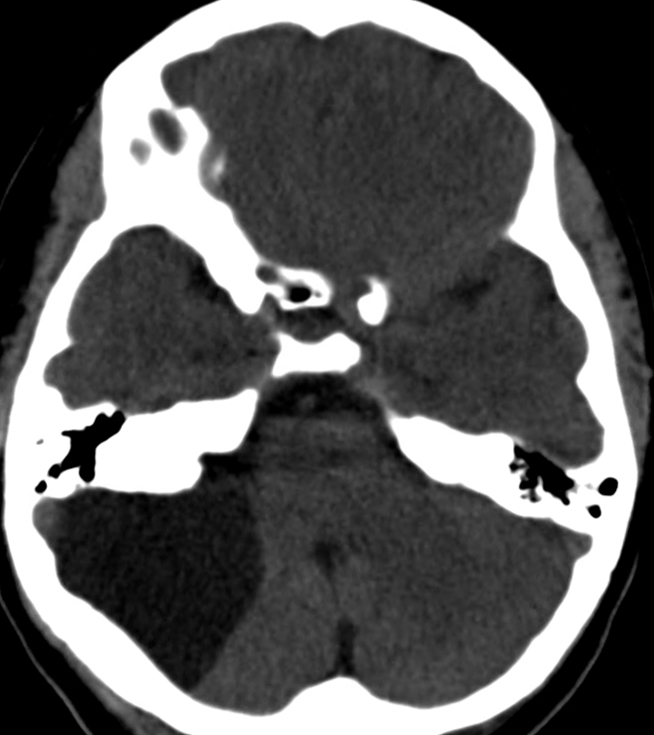
Figure 3: CT imaging demonstrates a low-density arachnoid cyst along the lateral aspect of the right cerebellar hemisphere. Other lesions, including low-grade tumors, may have a very similar appearance, and attention to the details of the lesion location, density, and pattern of enhancement is important in determining the true diagnosis.
BASIC DESCRIPTION
- Intracranial, extra-axial, cerebrospinal fluid (CSF)-containing cyst without communication to the ventricular system
- Accounts for 1% of all intracranial masses
PATHOLOGY
- Originates from embryonic meninges that fail to fuse during Sylvian fissure development
- CSF contents may arise from unidirectional inflow (ball-valve mechanism) versus secretion by cells lining AC wall
- Wall may contain ciliated cells, arachnoid tissue, or fibrous connective tissue
- Usually sporadic
- Rare association with Aicardi and Pallister-Hall syndromes
- Associated with temporal lobe hypoplasia, subdural hematomas, foramen of Monro, and/or aqueductal stenosis
- No inflammatory or neoplastic features
CLINICAL FEATURES
- Affects all ages
- Male gender predilection
- Common presenting signs/symptoms: range from asymptomatic/incidental finding to headache, sensorineural hearing loss, obstructive hydrocephalus
- Gradual enlargement is typical
- Treatment
- Most require no treatment
- Surgical resection, fenestration, and/or shunting for larger, symptomatic ACs
IMAGING FEATURES
- General
- Well-marginated extra-axial cyst which follows CSF density/signal intensity
- Mass effect and displacement of adjacent cortex
- Size variable
- Middle cranial fossa >> cerebellopontine angle cistern, suprasellar cisterns
- CT
- CSF-density, extra-axial mass
- ±Adjacent bony remodeling
- No enhancement on contrast-enhanced CT
- MRI
- T1-weighted imaging (T1WI): isointense to CSF
- T2-weighted imaging (T2WI): isointense to CSF
- FLAIR: complete drop-out of signal (just like CSF)
- DWI: no diffusion restriction
- T1WI+C: no enhancement
IMAGING RECOMMENDATIONS
- MRI without and with intravenous contrast (to exclude other lesions), including FLAIR and DWI
For more information, please see the corresponding chapter in Radiopaedia.
Contributor: Rachel Seltman, MD
References
Adeeb N, Deep A, Griessenauer CJ, et al. The intracranial arachnoid mater: a comprehensive review of its history, anatomy, imaging, and pathology. Childs Nerv Syst 2013;29:17–33. doi.org/10.1007/s00381-012-1910-x.
Boutarbouch M, El Ouahabi A, Rifi L, et al. Management of intracranial arachnoid cysts: institutional experience with initial 32 cases and review of the literature. Clin Neurol Neurosurg 2008;110:1–7. doi.org/10.1016/j.clineuro.2007.08.009.
Helland CA, Wester K. A population-based study of intracranial arachnoid cysts: clinical and neuroimaging outcomes following surgical cyst decompression in children. J Neurosurg 2006;105(5 Suppl):385–390. doi.org/10.3171/ped.2006.105.5.385.
Olaya JE, Ghostine M, Rowe M, Zouros A. Endoscopic fenestration of a cerebellopontine angle arachnoid cyst resulting in complete recovery from sensorineural hearing loss and facial nerve palsy. J Neurosurg Pediatr 2011;7:157–160. doi.org/10.3171/2010.11.PEDS10281.
Osborn AG, Salzman KL, Jhaveri MD. Diagnostic Imaging (3rd ed). Elsevier, Philadelphia, PA; 2016.
Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology 2006;239:650–664. doi.org/10.1148/radiol.2393050823.
Rabiei K, Tisell M, Wikkelsø C, Johansson BR. Diverse arachnoid cyst morphology indicates different pathophysiological origins. Fluids Barriers CNS 2014;11:5. doi.org/10.1186/2045-8118-11-5.
Sinha S, Brown JIM. Familial posterior fossa arachnoid cyst. Childs Nerv Syst 2004;20:100–103. doi.org/10.1007/s00381-003-0808-z.
Please login to post a comment.



