

Situation Awareness


INTRODUCTION
Situation awareness (SA) is a state of knowledge that arises from perceiving one’s own environment, comprehending the circumstances, and predicting what will occur next. SA has been described as simply “knowing what is going on around you,” with the attendant maxim, “What? So what? Now what?”
Rooted in the fields of military operations and aviation, SA was introduced into the medical lexicon by anesthesiologists in the 1990s and has been recognized as an essential nontechnical skill for surgeons of all disciplines. This article briefly summarizes the history and conceptual framework of SA and discusses its role in the neurosurgical operating room (OR). Behavioral heuristics that facilitate SA are explored, and factors that impede SA are highlighted as pitfalls.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
WHAT IS SITUATION AWARENESS?
Situation awareness is defined as “the perception of elements of the environment within a volume of time and space, the comprehension of their meaning, and the projection of their status in the near future” (Endsley 1988). Going beyond the lower-level processes of “focusing” or “paying attention,” SA is a mental state describing one’s internal representation of objects, relationships, and events as a situation unfolds over time (Schulz et al, 2013).
Although SA traces its origins to World War I–era military vernacular, the concept entered the scientific mainstream through applications in commercial and military aviation (Endsley 2015). During critical flight operations (eg, landing), pilots are thrust into a fast-paced setting in which any misjudgment could be fatal. To perform the action safely and efficiently, pilots must process vast quantities of data, update their situational assessment in relation to the task goals, and prepare for what might happen next. Mica Endsley, an engineer and former chief scientist of the US Air Force, represented this process in terms of the following 3 mental “levels” of SA (Endsley 1988, 1995a, 1995b) (Fig. 1):
- (Level 1 SA): Perception of elements in the current situation. This ground-level process involves gathering task-related information from the environment via observation, communication, direct measurement, etc. Information sources can include instruments, visual displays, alerts, and coworkers, among countless others.
- (Level 2 SA): Comprehension of the current scenario. At this level, raw data are synthesized into an understanding of the situation. This interpretation step is influenced by one’s knowledge base, expectations, goals, etc. An actionable judgment about themeaningof the data in relation to the task goal is made (“According to our altitude and speed, the approach angle is too shallow.”).
- (Level 3 SA): Projection of future status. Informed by the understanding of the current situation, a prediction is made about what is likely to happen next. Projections can be driven by intuition, logic, past experiences in similar situations, etc. Forming accurate predictions is critical for producing anticipatory actions to prevent an undesired event before it occurs.
As with other cognitive processes, SA is limited by the finite capacity of working memory, the fallibility of long-term memory, cognitive biases, and the obscuring effects of fatigue, illness, and malnutrition, among many others (seeFailures of SA). An individual’s SA can be influenced further by features of the environment, including ambient distraction, quality of the team, availability of resources, arrangement of the room, etc (see Human Factors and Ergonomics). Finally, individual SA should be distinguished from the related notion ofteam SA, which encompasses the actions and goals of a collective group.
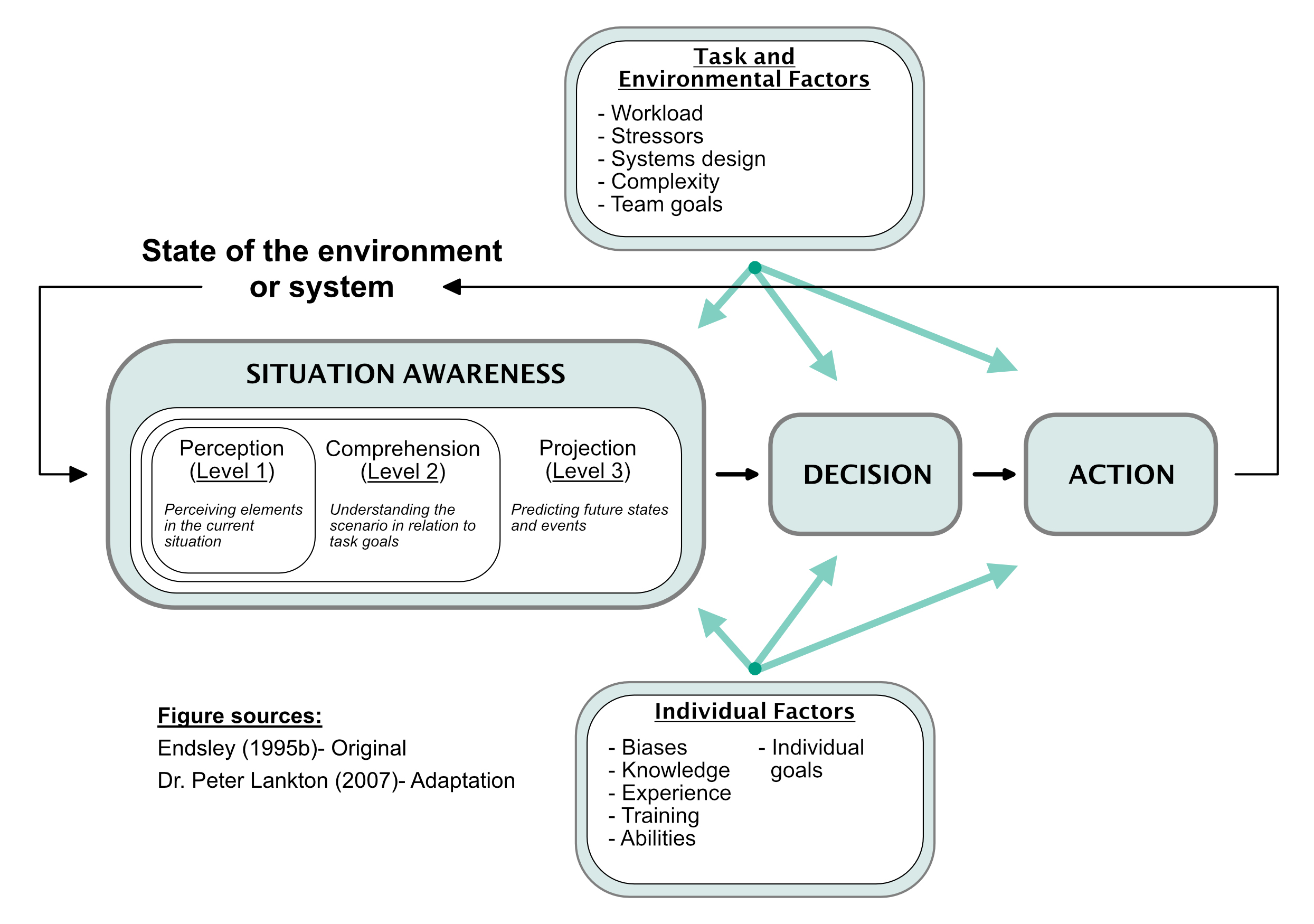
Figure 1: Endsley’s 3-level model of SA. Summarization of the model presented by Endsley (1995b) and Endsley et al (2015).
SITUATION AWARENESS IN THE OR
Background
Surgeons perform complex tasks that demand high levels of SA. Much like an airplane cockpit, the OR is a complex ecosystem of humans and devices working in harmony to accomplish a task. Maintaining a mental representation of an operation requires attending to many situational elements that can change frequently, instantly and unexpectedly throughout the procedure.
Poor SA is widely cited as a major contributor to adverse medical and surgical outcomes and SA is listed as 1 of the 4 following key nontechnical skills in the nontechnical skills for surgeons (NOTSS) taxonomy:
- Situation awareness
- Decision-making (please see the Surgical Decision-Making chapter)
- Communication and teamwork
- Leadership (please see the Leadership chapter)
To frame our discussion of SA in the neurosurgical OR, we present the following case vignette.
Surgical Vignette
A 9 year–old boy with several months of progressive hemiparesis presents for endoscopic biopsy of an exophytic medullary lesion. Dr M is the pediatric neurosurgeon who will perform the procedure along with a junior resident. The biopsy is booked for the navigation-equipped operating suite. Dr M has been on call for several days and asks the junior resident to prepare the patient while she performs her rounds.
The resident positions the patient prone, fixes him with cranial pins, rotates the operating table, and orients the endoscopy monitors. Dr M discusses the critical stages of the procedure with the anesthesiology team. The electrophysiologist places electrodes on the patient to monitor his sensory, motor, and brainstem auditory evoked responses. Dr M calls for a surgical time-out to confirm the case details and address any questions. Dr M and her resident perform a small suboccipital craniotomy to access the posterior fossa. After durotomy, Dr M dissects the cerebellar tonsils and passes an angled endoscope into the fourth ventricle.
As Dr M and the resident visualize the tumor, she asks for the OR music to be turned down and for nonessential conversation to stop. The patient’s vital signs are checked, and the electrophysiologist confirms that evoked responses are at baseline. Dr M notifies the anesthesia team as the resident obtains a biopsy specimen.
The patient’s evoked potentials are checked once more, and no changes from baseline are indicated. Closure is performed. Dr M again calls for a time-out before the patient is taken to the recovery room. The patient recovers without any neurological deficits. Histopathology reveals a low-grade glial tumor.
Situational Elements
In this medullary biopsy case, the neurosurgeon must track at least 4 key situational elements to construct a mental model of the surgery (Table 1), as follows:
- Patient: The patient and his family are the focus of the operation. Static attributes of the patient include his demographic details, medical history, baseline physical examination results, medications/allergies, previous surgeries, etc. This information is generally elicited during the preoperative visit. In the OR, many dynamic attributes come into view, such as the patient’s physiological status and vital signs. Considering the location of the tumor, these attributes are subject to instantaneous fluctuations and may call for emergent intervention. In the process of data gathering, comprehension, and projection, the neurosurgeon must understand the following:
- What sources of information are available? (eg, electrophysiological monitoring)
- How is the information accessed? (eg, asking the technician to run motor potentials)
- How is the information interpreted? (eg, functioning of brainstem nuclei)
- What actions should be taken in response to the information? (eg, avoid critical structures during biopsy)
- Neurosurgeon (self): The neurosurgeon herself is a complex actor in this scenario with a number of static and dynamic characteristics. The static variables include Dr M’s medical knowledge, baseline technical abilities, experience with similar cases, etc. The interaction between experience and Endsley’s 3-level model is illustrated in Fig. 2. Dynamic factors that influence the neurosurgeon’s performance include possible fatigue (she is on call), nourishment, task engagement, perception of how the case is going, and distractions (eg, the floor patient whose mental status is deteriorating).
The main source of insight about the neurosurgeon’s status is introspection. Ample research from cognitive science has found limitations in human introspection when it comes to interpreting our feelings and explaining our actions (Pronin 2007). For example, if a patient of hers recently suffered neurological complications after a brainstem biopsy, the surgeon’s decision-making might be affected at the conscious or subconscious level. Being mindful of these possible biases can help prevent errors in perception, judgment, and projection and thus constitutes an important element of SA. - Environment: Monitoring the OR ecosystem can be difficult, especially during critical stages of a surgery. Aside from certain physical attributes and permanent fixtures in the room, almost everything about the OR environment is dynamic; people enter and exit the room, multiple conversations ensue, alarms come in and out of register, and shift changes usher in new personnel. In the vignette above, the neurosurgeons try to optimize the environment to suit their objectives.
They book the neuronavigation suite to help localize the tumor. They ask for assistance from their electrophysiologist colleagues to monitor brainstem function. The resident rotates the operating table to maximize the workspace and conveniently positions the endoscopy monitor. Dr M requests quiet during the crux of the procedure, much like those who follow the “sterile cockpit” regulations that prohibit all nonessential conversations during critical airline operations (McIlhenny 2018). Still, some environmental factors (eg, whether the scrub nurse most experienced with Dr M’s posterior fossa cases is on service) might be outside their control. - Tasks: The goal of the surgery needs to be considered from the individual and team perspectives. Each team member has specific objectives that support the broader team goal. At a minimum, team members need to understand how their individual objectives support the overall team goal. Dr M’s immediate objectives may include obtaining the tissue biopsy specimen and educating her trainee. However, functioning as team leader, Dr M should be familiar with all individual objectives so that she can recognize the proximal and future effects of the team’s actions, identify mistakes, and steer the operation back on course.
Aligning individual tasks in the direction of the team goal requires constant and effective communication. The neurosurgeon in this vignette demonstrates this aspect of SA by calling for 2 surgical time-outs to ensure that everyone is on the same page. She also alerts the anesthesiologist before performing the biopsy in anticipation of sudden changes in the patient’s condition, which helps the anesthesiologist monitor the patient’s physiologic status and supports the team goal of performing a safe biopsy.
| Situation | Perioperative Elements | |
| Static | Dynamic | |
| Patient |
Name Sex Height/weight Position (head fixation) |
Heart rate Blood pressure Temperature Evoked responses Depth of anesthesia Anatomy (modified by surgery) |
| Neurosurgeon |
Medical knowledge Quality of training Years of experience Technical skill Leadership abilities |
Retrieval of medical knowledge Energy and concentration level Confidence throughout operation |
| Environment |
Hospital Operating room Fixed equipment Facility resources |
Unrelated conversation Ambient noise/music OR personnel (rotating scrub nurse, shift change, etc) |
| Individual | Team | |
| Tasks |
Neurosurgeon Perform safe tissue biopsy Educate residents and trainees Anesthesiologist Administer anesthetic Secure airway Maintain physiologic stability Electrophysiologist Monitor evoked responses Nursing team Assist in case preparation Maintain sterile surgical field Handle biopsy specimen Pass instruments Update patient’s family |
Obtain medullary biopsy specimen in a safe and efficient manner
|


Figure 2: Interaction effect between surgical expertise and nontechnical skill, mapped onto Endsley’s 3-level model. The gap between an experienced surgeon and a junior resident increases with higher levels of SA, producing the “expertise interaction.”
Promoting SA in the OR
Several steps can be taken to promote SA in the OR. A more extensive discussion is available from Flin and Paterson-Brown (2015). Constructive practices include the following:
- Communication: Active communication among providers is the bedrock of collaborative medicine, and miscommunication is a leading source of medical errors that ultimately harm patients (Bates et al, 1997). Ensuring that all team members are briefed on the patient and the procedure solidifies the team goal. Inviting questions before the procedure can bring new information to the surgeon’s attention and will empower the OR team to speak up if (or, ideally, before) problems arise. A formal briefing should occur before the first incision, but providing frequent progress updates keeps the surgery moving and ensures that everyone stays informed.
- Visualization: Surgeons benefit from visualizing every step of the surgery from start to finish, asking, “What do I expect things to look like? Which instruments will I use? What challenges might we encounter? Do we have access to the resources we would need? Can I help prepare other team members for the unexpected?” Having a clear mental image of the entire process helps the surgeon recognize when a procedure is deviating off course.
Visualization also forms the basis of effective contingency planning. Depending on the likelihood and severity of these contingency scenarios, the surgeon may wish to mobilize resources or make certain that they are available. Communicating the surgeon’s expectations to other team members allows everyone to prepare for how they would respond in that scenario. - Trust, accountability, and teamwork: Surgeons feel a deep responsibility for all aspects of their patients’ care. However, many components of a successful operation fall outside the neurosurgeon’s expertise (eg, securing the airway). Showing deference to other practitioners and acknowledging their skillset helps foster an environment of trust. Teams that operate from a place of mutual respect are less likely to suffer breakdowns in team SA.
- Time management: The neurosurgeon must maintain a balance between safety and efficiency in the OR. As his or her technical proficiency increases, the surgeon can work quickly through routine aspects of a procedure without jeopardizing patient safety. In the example vignette, the Dr M recognizes the need to work efficiently through the beginning stages to avoid any time pressures during the biopsy.
Good time management is the result of excellent planning and mobilization of resources before they are needed. Teams that operate with a shared mental model of the procedure and its various component steps are able to function more efficiently.
Green et al (2017) proposed the “SLAM” mnemonic to outline the following 4 steps toward improving SA:
- Stop: Think through the task from start to finish.
- Look: Ask yourself, “Is anything out of the ordinary?”
- Assess: “Are things going as expected? Are we on track? Am I prepared for the unexpected?”
- Manage: Address concerns or issues, regroup, discuss with the team, and prepare for what is next.
Human Factors and Ergonomics
Systems and environments can be engineered to promote SA. Human factors and ergonomics (HFE) is a discipline focused on optimizing the way in which humans interact with other humans, machines, technology, and the environment. Simply put, HFE deals with creating environments that facilitate productive behaviors and impede counterproductive behaviors, thereby maximizing SA. Many researchers have studied HFE principles in relation to surgical performance (Graafland et al, 2015). Individual and team SA is facilitated by the following HFE-inspired practices (Joint Commission, 2015):
- Adhering to safety regulations (eg, mandating a surgical time-out, using 2-factor patient identification)
- Using computerized automation (eg, programmed infusion pumps for safe medication delivery)
- Following procedure checklists (eg, confirming all planned steps before the procedure begins)
- Scheduling (eg, aligning shifts to decrease turnover during the procedure, reducing burnout)
- Communicating (eg, repeating instructions to ensure that they were properly understood)
- Reducing distractions (eg, turning down OR music, minimizing nonessential conversation)
- Laying out the room (eg, displaying MRIs conveniently in the surgeon’s view, positioning the microscope in a way that maximizes usability)
- Systematically instituting quality improvement (eg, scheduling time for team reflection and feedback)
FAILURES OF SA
Situation awareness is a multifactorial process, and breakdowns of SA usually have multiple causes. Miscommunication, ineffective leadership, and poor human factors design undoubtedly contribute to poor SA in the OR. Situation awareness depends on error-prone cognitive systems, such as perception, working memory, and long-term memory that must be able to coordinate both “top-down” and “bottom-up” inputs.
At Endsley’s first level (perception), for example, the surgeon’s perceptual attention is guided by bottom-up features of the environment (eg, the saliency of a bleeding vessel) and top-down influences (eg, the patient’s decreasing blood pressure causes the surgeon to look for hemorrhage). The cognitive system is also vulnerable to a host of well-known biases, including the following:
- Anchoring bias: Anchoring is the tendency to let an initial impression unduly influence subsequent thinking. Anchoring is one reason why a misdiagnosis is difficult to correct. Once a diagnosis is proposed, surgeons might misperceive or overlook clues that point toward an alternative diagnosis. Anchoring bias is closely related to (but distinct from) confirmation bias, which is the tendency to seek and interpret evidence in support of pre-existing beliefs.
To detect anchoring and confirmation biases, surgeons must constantly re-evaluate the situation and ask whether other explanations need to be considered. Soliciting input from colleagues is another way to counteract our individual biases, but it should be noted that confirmation and anchoring biases can exist at the group, department, and institution levels. - Cognitive tunneling: Tunneling, also known as inattentional blindness or selective attention, is an inability to see something that is plainly in view. In the following video demonstration Daniel Simons, PhD, and his colleagues asked viewers to count the number of passes made by a basketball team. Although most people were able to count the passes, fully half of the participants missed the woman in a gorilla costume who sauntered through the center of the action.
In the OR, surgeons must filter out distracting information to focus on the operative task, but that can come at the cost of missing important cues. Tunneling is likely influenced by the difficulty of the task and the experience level of the surgeon. With good preoperative visualization, the surgeon develops a sense of what to look out for during the procedure, which might raise the salience of an otherwise mundane but consequential piece of information.
- Cognitive overload: Situation awareness can break down when cognitive resources are exhausted. Experienced surgeons with expertise in their discipline will be less cognitively taxed than a junior trainee, which enables them to allocate more resources toward maintaining their SA. For a graphic illustration of how expertise interacts with SA, see Fig. 2.
CONCLUSIONS
- Situation awareness is the state of perceiving information in the environment, understanding its meaning, and predicting what will come next.
- Breakdowns of SA contribute to medical error and can be caused by miscommunication, poor leadership, suboptimal workplace design, and cognitive errors.
- Behaviors that facilitate SA include preoperative briefings, visualization, contingency planning, and time management.
Contributor: Samuel B. Tomlinson, BA
References
Afkari H, Bednarik R, Mäkelä S, Eivazi S. Mechanisms for maintaining situation awareness in the micro-neurosurgical operating room. Int J Hum Comput Stud 2016;95:1–14. https://doi.org/10.1016/j.ijhcs.2016.05.004.
Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. JAMA 1997;277:307–311. https://pubmed.ncbi.nlm.nih.gov/9002493/.
Endsley MR. Design and evaluation for situation awareness enhancement. Proc Hum Factors Ergon Soc Annu Meet 1988;32;97–101. https://doi.org/10.1177/154193128803200221.
Endsley MR. Measurement of situation awareness in dynamic systems. Hum Factors 1995a;37:65–84. https://doi.org/10.1518/001872095779049499.
Endsley MR. Toward a theory of situation awareness in dynamic systems. Hum Factors 1995b;37:32–64. https://doi.org/10.1518/001872095779049543.
Endsley MR. Situation awareness misconceptions and misunderstandings. J Cogn Eng Decis Mak 2015;9:4–32. https://doi.org/10.1177/1555343415572631.
Fischer MA, Kennedy KM, Durning S, et al. Situational awareness within objective structured clinical examination stations in undergraduate medical training—a literature search. BMC Med Educ 2017;17:262. https://doi.org/10.1186/s12909-017-1105-y.
Flin R, Paterson-Brown S. Situation awareness. In Flin R, Youngson GG, Yule S (eds), Enhancing Surgical Performance. CRC Press, Boca Roton, FL; 2015:63–81. https://doi.org/10.1201/b18702.
Graafland M, Schraagen JMC, Boermeester MA, et al. Training situational awareness to reduce surgical errors in the operating room. Br J Surg 2015;102:16–23. https://doi.org/10.1002/bjs.9643.
Green B, Parry D, Oeppen RS, et al. Situational awareness—what it means for clinicians, its recognition and importance in patient safety. Oral Dis 2017;23:721–725. https://doi.org/10.1111/odi.12547.
Greenberg CC, Regenbogen SE, Studdert DM, et al. Patterns of communication breakdowns resulting in injury to surgical patients. J Am Coll Surg 2007;204:533–540. https://doi.org/10.1016/j.jamcollsurg.2007.01.010.
Joint Commission. Human factors analysis in patient safety systems. Available at: https://www.jointcommission.org/assets/1/6/HumanFactorsThe_Source.pdf. Accessed November 11, 2018.
McIlhenny C. Human factors and patient safety in surgery. In Paterson-Brown S, Paterson H (eds), Core Topics in General & Emergency Surgery, 6th Ed. Elsevier Science Publishing Company, New York, NY; 2018:114–121.
Mishra A, Catchpole K, Dale T, McCulloch P. The influence of non-technical performance on technical outcome in laparoscopic cholecystectomy. Surg Endosc 2008;22:68–73. https://doi.org/10.1007/s00464-007-9346-1.
Pronin E. Perception and misperception of bias in human judgment. Trends Cogn Sci 2007;11:37–43. https://doi.org/10.1016/j.tics.2006.11.001.
Schulz CM, Endsley MR, Kochs EF, Gelb AW, Wagner KJ. Situation awareness in anesthesia: concept and research. Anesthesiology 2013;118:729–742. https://doi.org/10.1097/ALN.0b013e318280a40f.
Way LW, Stewart L, Gantert W, et al. Causes and prevention of laparoscopic bile duct injuries: analysis of 252 cases from a human factors and cognitive psychology perspective. Ann Surg 2003;237:460–469. https://doi.org/10.1097/01.SLA.0000060680.92690.E9.
Yule S, Flin R, Paterson-Brown S, Maran N. Non-technical skills for surgeons in the operating room: a review of the literature. Surgery 2006;139:140–149. https://doi.org/10.1016/j.surg.2005.06.017.
Please login to post a comment.




