Fourth Ventricular Tumors


This is a preview. Check to see if you have access to the full video. Check access
Resection of a Fourth Ventricular Ependymoma Adherent to the Floor of the Ventricle
Fourth ventricular tumors pose a surgical challenge, albeit less than their third ventricular counterparts, because of their relation to the brainstem; this relation can vary from simply displacement to invasion.
This technical challenge is further complicated because the tumor is often concealed by key cerebellar structures, including the cerebellar tonsils and hemispheres or the vermis. Tumors may involve adjacent structures through extension via the foramen of Luschka and by reaching the premedullary, cerebellomedullary, prepontine, and anterior spinal cisterns.
The major structures that compose the borders of the fourth ventricle along the craniocaudal extent are:
- Anteriorly (floor): midbrain, pons, medulla
- Laterally: superior, middle, and inferior cerebellar peduncles
- Superiorly (roof): superior medullary velum, cerebellar lingula, fastigium
- Inferiorly (roof): choroid plexus, tela choroidea, inferior medullary velum, cerebellar uvula, and nodulus
Tumors of the fourth ventricle commonly originate from the following structures composing the floor: the ependyma, choroid plexus, and tela choroidea. Lesions may also arise outside the ventricle and secondarily extend into this chamber, including medullary, tectal, and cerebellar hemispheric masses. These lesions are thus accessible via a fourth ventricular approach.
Importantly, preoperative magnetic resonance imaging (MRI) may be inconclusive with regard to the presence of brainstem invasion, and in fact, it can often be falsely indicative of invasion. Many fourth ventricular tumors, particularly those with an exophytic growth pattern, have a vascularized pedicle and demonstrate compression of the adjacent structures, but lack invasion.
Lateral extension into the fourth ventricle’s outlets typically occurs in medulloblastomas, ependymomas, and gliomas. This extension may progress to involve the foramen of Luschka and even cerebellopontine angle cisterns. This tumor configuration can facilitate cranial nerve involvement via tumor impingement or encasement. Similarly, caudal extension may progress via the obex to affect the superior cervical spinal cord and produce upper cervical myelopathy or even radiculopathy.

ATLAS Choice Bipolar Forceps
Designed for your every surgical maneuver
Five tip sizes for brain and spine procedures
Unparalleled non-stick and low-profile features
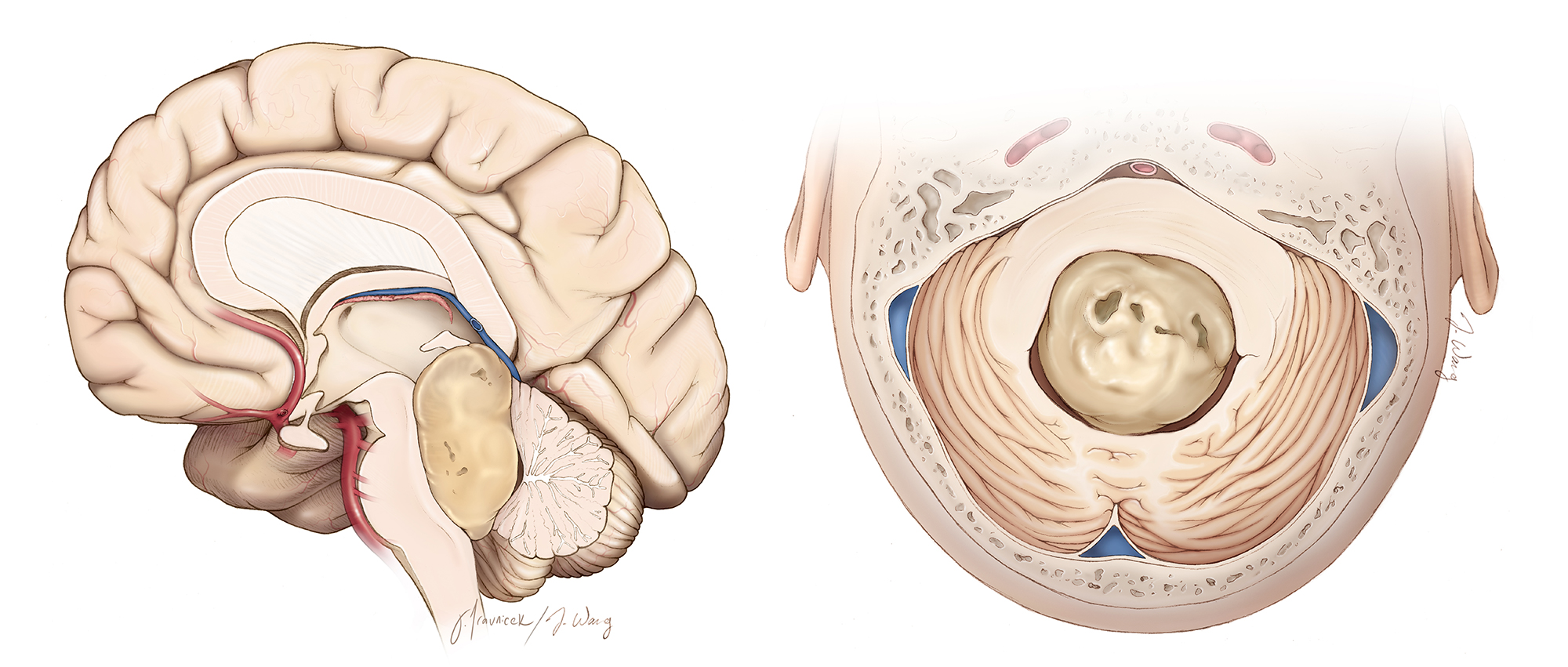
Figure 1: The typical location of a fourth ventricular tumor is demarcated. The surgical target is covered by the vermis and hemispheres. The tumor may extend to the level of the pineal region, requiring a combined telovelar and supracerebellar approach. Most large tumors can be resected via the telovelar route alone. Invasion of the floor is the limiting factor in achieving gross total resection (Redrawn from Tew, van Loveren, Keller*).
Diagnosis and Evaluation
For a general discussion of diagnosis and evaluation for ventricular tumors, see the Principles of Intraventricular Surgery chapter where Table 1 provides a summary of radiologic features consistent with each tumor type.
Hydrocephalus and gait ataxia are common symptoms and signs. Dysmetria and dysdiadochokinesia are possible with laterally located tumors. Less common signs include diplopia, facial weakness, and lower cranial nerve dysfunction. Commonly encountered in the fourth ventricle are ependymomas, medulloblastomas, epidermoid cysts, pilocytic astrocytomas, hemangioblastomas, and cavernous malformations. For a more detailed description of these tumors, see the Ventricular Tumors chapter.

Figure 2: A typical ependymoma is shown. Note the partial encasement of the posterior inferior cerebellar artery (PICA) branches within the lateral aspects of the tumor (arrows). The tumor is partially enhancing and appears to be adherent to or invading the floor.
Indications for Surgery and Preoperative Considerations
For a general discussion of the indications for surgery and preoperative considerations for patients with ventricular tumors, see the Principles of Intraventricular Surgery chapter.
Neurophysiologic monitoring is recommended if manipulation of the brainstem or any of the cranial nerves is expected. Brainstem auditory evoked responses (BAERs) are highly sensitive to early signs of brainstem dysfunction. Fluctuation in vital signs may occur during manipulation of the floor and is a serious warning sign to halt retraction and dissection in the area.
Operative Anatomy
The vascular structure most pertinent to a fourth ventricular approach is the posterior inferior cerebellar artery (PICA).

Click here to view the interactive module and related content for this image.
Figure 3: There are five segments of the PICA: anterior medullary, lateral medullary, tonsillomedullary, telovelotonsillar, and the cortical segments. Knowledge of the anatomic distribution of these segments is critical to successful navigation of the fourth ventricle and resection of the tumor. The first three branches listed are particularly important as they give rise to feeding vessels to the brainstem and tumors. Establishment of the arterial anatomy preoperatively is important for lessening the risk of ischemic injury. Tumors may also involve the vasculature of the choroid plexus or tela choroidea (image courtesy of AL Rhoton, Jr).
Up to 20% of PICAs originate from the vertebral artery extradurally. This anatomical variant should be considered during the extradural dissection of the vertebral artery at the craniocervical junction. The caudal loop of PICA encompasses the segment of the PICA between the lower cranial nerves and the pole of the tonsil. The cranial loop of the PICA courses between the rostral pole of the tonsil and the inferior medullary velum.
Click here to view the interactive module and related content for this image.
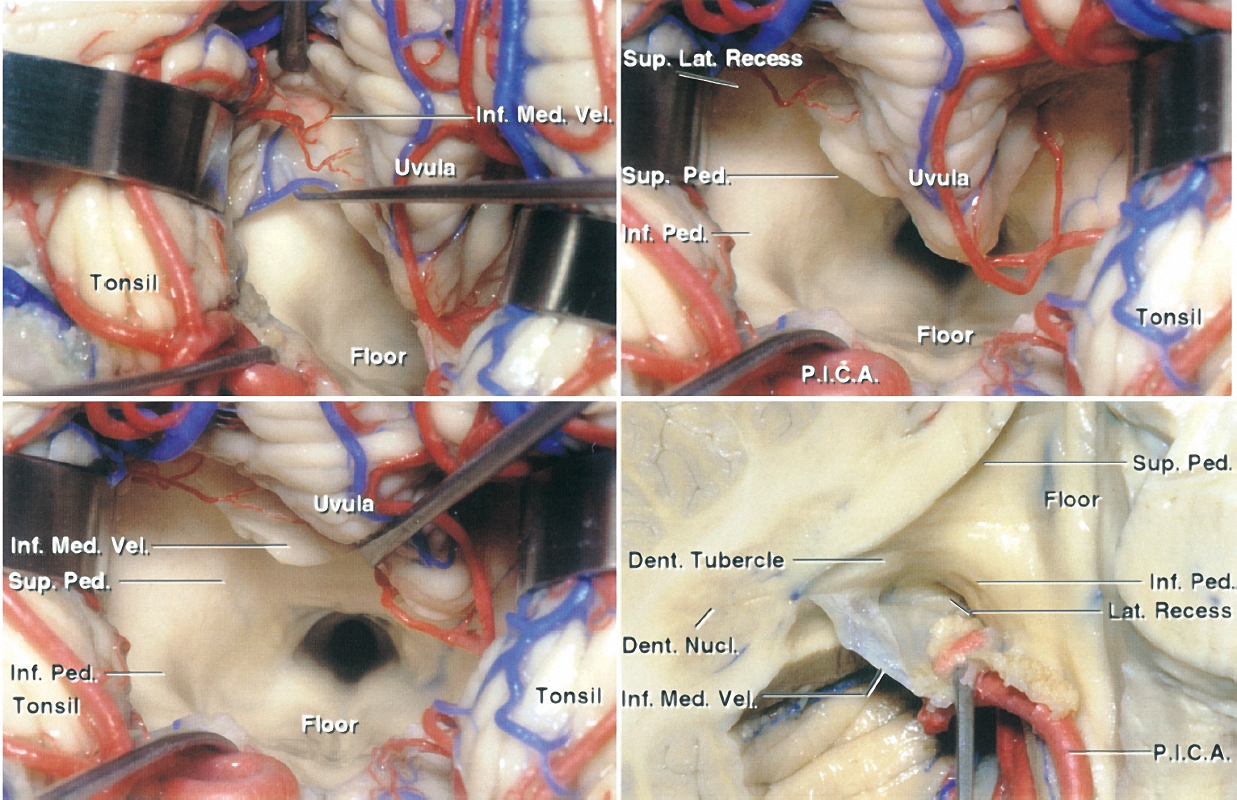
Figure 4: The basic principles of the telovelar approach are shown. Note the path of dissection medial to the tonsil and lateral to the vermis. A wide exposure of the ventricle is possible through an inferior-to-superior trajectory (images courtesy of AL Rhoton, Jr). For further details, please refer to chapter on telovelar approach.

Click here to view the interactive module and related content for this image.
Figure 5: The topography of the eloquent fourth ventricular floor is mapped. The locations of the facial colliculus, as well as the hypoglossal and vagal triangles, are evident. Stimulation mapping can effectively guide the surgeon to avoid these critical structures during surgery of the floor (images courtesy of AL Rhoton, Jr).
MICROSURGICAL RESECTION OF FOURTH VENTRICULAR TUMORS
Historically, the approach to fourth ventricular tumors involved either cerebellar hemisphere resection or vermian split. Vermian split syndrome is characterized by neurobehavioral abnormalities, imbalance, and cerebellar mutism. In an attempt to avoid these untoward side effects, an alternative approach has been designed.
The telovelar (transcerebellomedullary fissure) approach is flexible and allows resection of most lesions in this area. It facilitates generous exposure of most of the fourth ventricular space, with minimal disruption of the normal structures. For more details, please refer to the chapter on Telovelar Approach in the Cranial Approaches volume.

Figure 6: A limited suboccipital craniotomy is conducted with the patient in the lateral position (left “down”). The dura is incised in a Y-shaped fashion. A linear dural opening is an option for purely midline lesions; compared to the “Y” dural incision, the linear one can be readily closed in a watertight fashion. The C1 lamina is marked with an arrow.
INTRADURAL DISSECTION
Initial opening of the arachnoid layers covering the cisterna magna achieves desirable brain relaxation.

Figure 7: The telovelar approach provides the least invasive and most effective route to the fourth ventricle.

Figure 8: A small inferior vermian split is often safe for exposure of large cranially situated fourth ventricular tumors near the superior medullary velum and the pineal region (top image). Alternatively, a combined telovelar and supracerebellar approach may be attempted (bottom illustration).
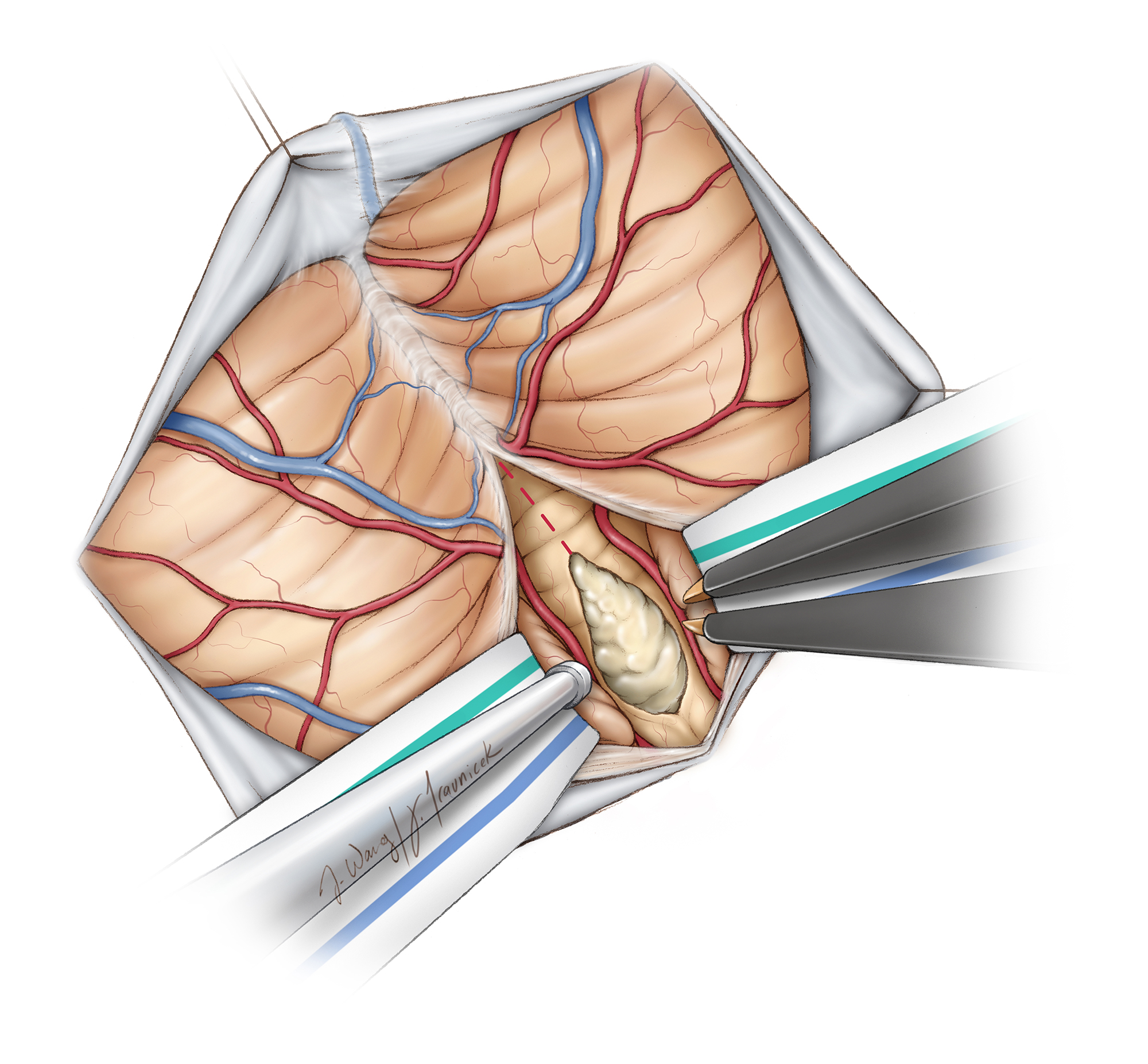
Figure 9: Optimal working angles for large or superior fourth ventricular lesions can be expanded by craniodorsal retraction or minimal transection of the inferior vermis attenuated by the mass effect of the tumor.
The following steps may help simplify tumor resection:
- Microsurgical dissection of the PICA branches from the lateral and superior poles of the tumor protects the relevant vasculature. These arteries provide feeding perforators to the tumor. These perforators must be carefully isolated, coagulated, and shapely cut. Blunt avulsion injury to these vessels places the parent arteries at risk.
- Next, the tumor is internally debulked while avoiding inadvertent penetration of the capsule. The plane of floor of the ventricle may be approximated by gentle elevation of the inferior pole of the tumor to inspect the degree of the floor’s tumor infiltration.
- Tumor enucleation allows the superior pole of the tumor to be rolled inferiorly; the egress of cerebrospinal fluid around this pole confirms entry into the fourth ventricle. This view over the superior pole allows me to approximate the level of the floor with respect to the anterior tumor capsule, further guiding tumor debulking.
- The superior pole and middle of the tumor are further debulked while the lateral poles are mobilized into the resection cavity.
- An ultrasonic aspirator is used to shave tumor off while leaving a thin sheet of tumor over the adherent areas of the floor. The floor is strictly protected and not manipulated.
Most tumors have insertion points along the brachium pontis and potentially the lateral recesses, but rarely along the midline. An ultrasonic aspirator is used to remove the middle section of the tumor, which can usually be lifted off readily from the midline floor.

Figure 10: The PICA-perforating arteries are severed (left image). Microsurgical debulking and circumdissection of the tumor is conducted (right image).
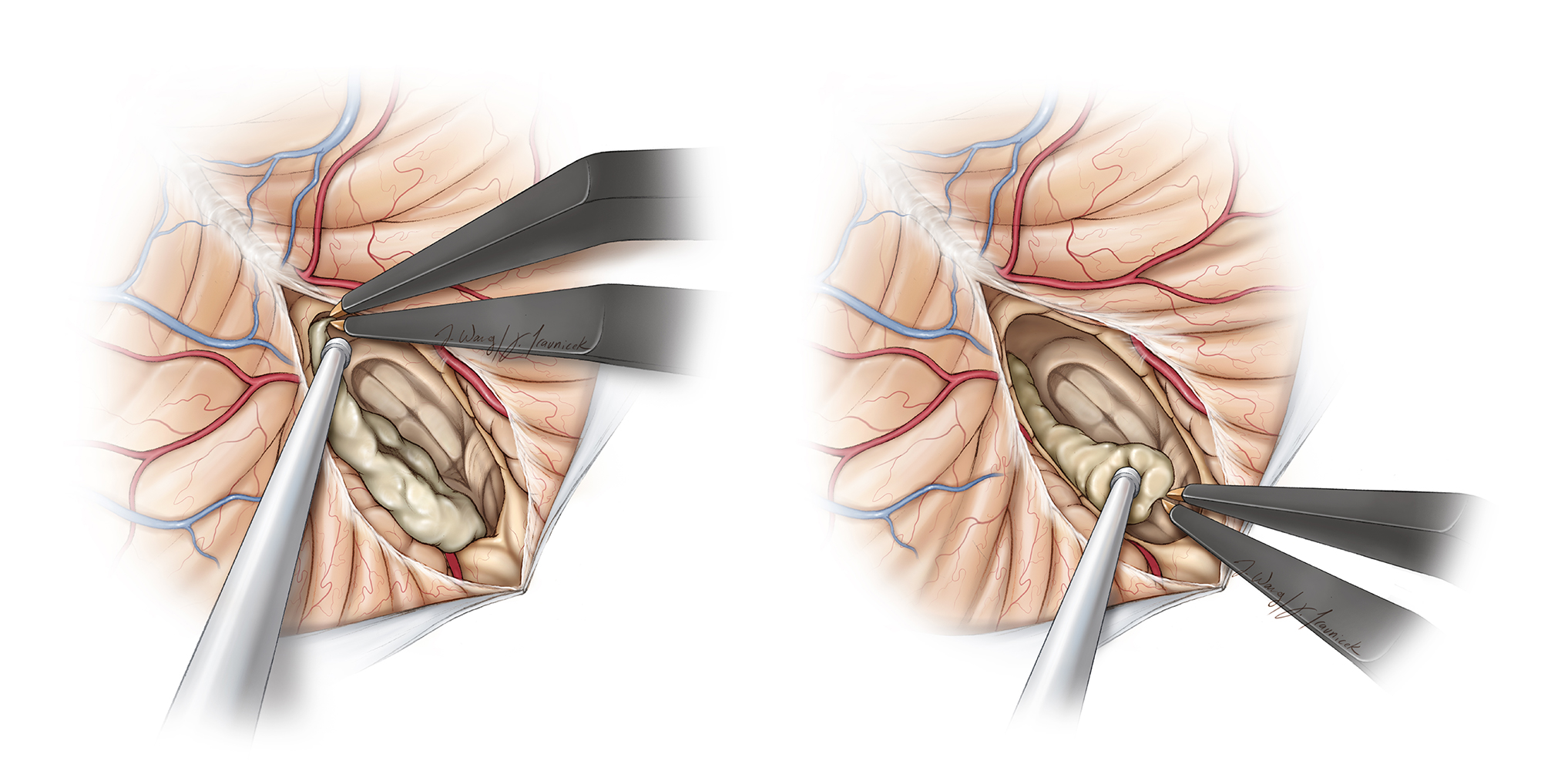
Figure 11: The superior pole of the tumor is debulked and mobilized (left image). Finally, the tumor along the floor is inspected (right image). Adherent tumor is left behind. Manipulation of the floor leads to significant mid to lower cranial nerve dysfunction and is not warranted (Redrawn from Tew, van Loveren, Keller*).

Figure 12: These intraoperative photos demonstrate the steps involved in resection of the ependymoma shown in Figure 2. The top two images show the tumor and microsurgical dissection of the right PICA. The bottom two images show tumor removal using ultrasonic aspiration while leaving a thin sheet of tumor over the infiltrated floor laterally (lower image-right brachium pontis).

Figure 13: The use of the telovelar approach for removal of a fourth ventricular dermoid (top MRIs-red arrow) is shown (middle photo). Following removal of the tumor contents, the adherent capsule is left on the floor and the entry into the aqueduct is apparent (lower photo).
Fourth Ventricular Dermoid Cyst
Closure and Postoperative Considerations
For a detailed discussion of recommendations for postoperative care of patients with ventricular tumors, see the Principles of Intraventricular Surgery chapter.
A watertight dural closure is necessary since the ventricle is entered within the posterior fossa. I recommend the use of a short course of postoperative steroids to minimize the risk of aseptic meningitis. The bone flap is replaced or a cranioplasty attempted.
Pearls and Pitfalls
- Aggressive manipulation of the floor of the ventricle is strictly avoided.
- Strategic tumor debulking and circumdissection based on the steps listed above is advised.
Contributor: Benjamin K. Hendricks, MD
*Redrawn with permission from Tew JM, van Loveren HR, Keller JT. Atlas of Operative Microneurosurgery, WB Saunders, 2001. © Mayfield Clinic
Related Materials
Available Through the Atlas
-

The long-term outcome after surgical treatment of dorsally exophy...
-
The pathophysiology of oral pharyngeal apraxia and mutism followi...
-
Ependymoma in childhood: Prognostic factors, extent of surgery, a...
-
Microsurgical Anatomy of the Extracranial-Extradural Origin of th...
-
Symptomatic subependymoma: A clinicopathological and flow cytomet...
-
Experiences with the telovelar approach to fourth ventricular tum...
Unavailable Through the Atlas
-

Brain stem mapping: Neurophysiological localization of motor nucl...
-
An analysis of factors determining the need for ventriculoperiton...
-
Second-look surgery for incompletely resected fourth ventricle ep...
-
Cerebellum and Fourth Ventricle
-
Intracranial ependymomas in adult patients: Analyses of prognosti...
-
Resection of fourth ventricle tumors without splitting the vermis...
-
Choroid plexus papillomas: A single institutional experience
-
Subependymomas: An analysis of clinical and imaging features
-
Surgery of intraventricular tumors
-
Combined treatment of fourth ventricle ependymomas: Report of 26...
-
Transient mutism following posterior fossa surgery in children
-
Telovelar approach: Technical issues for large fourth ventricle t...
-
Surgical approach to the fourth ventricle cavity through the cere...
-
Monitoring motor function during resection of tumours in the lowe...
-
Combined transventricular and supracerebellar infratentorial appr...
Please login to post a comment.