Transsylvian Selective Amygdalohippocampectomy



This is a preview. Check to see if you have access to the full video. Check access
Transsylvian Selective Amygdalohippocampectomy
A number of different surgical techniques are effective for treatment of drug-resistant medial temporal lobe epilepsy. Of these, transsylvian selective amygdalohippocampectomy (SA), which was originally developed to maximize temporal lobe preservation, is arguably the most technically demanding to perform. Recent studies have equivocally suggested that SA may result in better neuropsychological outcomes with similar postoperative seizure control as standard anteromedial temporal lobectomy and amygdalohippocampectomy (ATL), which involves removal of the lateral temporal neocortex. The anteromedial temporal lobectomy is discussed in its own dedicated chapter.
Because of the technical complexity of SA, presumed risks, and required familiarity with microsurgical techniques on the part of the surgeon, the use of SA has been limited compared with ATL. The narrow operative corridor through the transsylvian route requires that the surgeon be thoroughly familiar with the surgical anatomy of the region and handling of important adjacent cerebrovascular structures.
For diagnosis, evaluation, and preoperative considerations of medial temporal lobe epilepsy and its corresponding surgical indications, please refer to the Anteromedial Temporal Lobectomy chapter.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features

Figure 1: I prefer to use SA for tumors located within the amygdala, uncus, and anterior hippocampus, especially in the dominant hemisphere. I do not believe SA affords significant advantages over the standard anteromedial temporal lobectomy and amygdalohippocampectomy for medial temporal lobe sclerosis.
Operative Anatomy
The medial temporal lobe surgical anatomy is complicated and must be understood in its entirety before undertaking this procedure in order to avoid injury to the important adjacent cerebrovascular structures; most at risk are the middle cerebral artery (MCA) branches, the diencephalon/brainstem, the anterior choroidal artery, and the oculomotor nerve.
The angle of exposure of the ventricle can disorient the surgeon, and therefore intraoperative neuronavigation is helpful. All relevant boundaries of the structures at risk should be kept in mind. An imaginary line drawn from the MCA to the inferior choroidal point (defined approximately as the most anterior aspect of the choroid plexus where the anterior choroidal artery enters the ventricle) is a reliable border between the amygdala inferiorly and the globus pallidus superiorly. Medially, the amygdala extends to the level of the basal cisterns as the uncus, abutting the oculomotor nerve. The inferior portion of the amygdala makes up the anterior roof and wall of the temporal horn.
Both the head and body of the hippocampus can be identified within the anterior aspect of the temporal horn. The pes of the hippocampus forms the medial border of the anterior temporal horn, whereas the superior border contacts the posteroinferior border of the amygdala. The body of the hippocampus makes up the medial aspect of the temporal horn floor and is bordered laterally by the collateral eminence, which forms the lateral floor of the temporal horn.
The choroidal fissure, which lies between the choroid plexus (attached to the thalamus) and the fimbria, makes up the medial wall of the posterior two-thirds of the temporal horn. Opening the choroidal fissure provides access to the ambient cistern—this maneuver is avoided during this operation. Choroidal fissure is an important landmark in SA because all structures lying medial to the choroidal fissure belong to thalamus, whereas all structures lateral to it may be removed. Exposure of the MCA bifurcation, most importantly the temporal horn, and the choroid plexus orients the surgeon to the relevant anatomy.

Click here to view the interactive module and related content for this image.
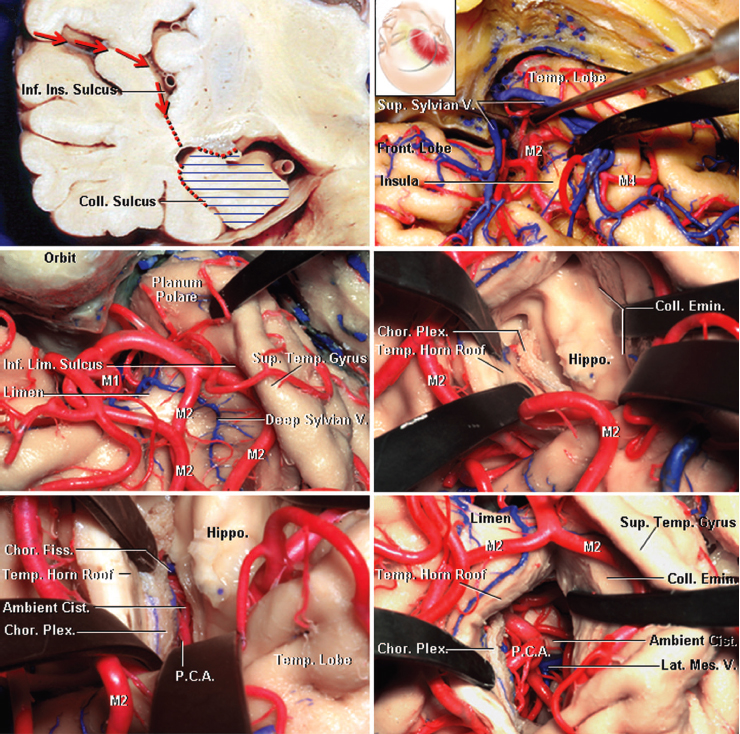
Figure 2: Operative anatomy for a right-sided SA is shown. Wide Sylvian fissure split exposes the limen insula, anterior part of the insula, the inferior insular sulcus, the temporal pole, and the M1 and M2 segments of the MCA (left upper image). The lateral part of the Sylvian fissure has been mobilized to expose the inferior insular sulcus posterior to the limen. The location of the amygdala deep to the floor of the Sylvian fissure is marked in green. Two incisions may be used to reach the amygdala and the temporal horn. The yellow line directly leads into the amygdala and the temporal horn and is associated with less risk of interrupting the optic radiations than the black line in the inferior insular sulcus (right upper image). The incision in the inferior insular sulcus exposes the head of the hippocampus, the choroidal fissure, and the anterior choroidal artery (left middle image). The right middle image provides a view of the limen insula when the MCA branches are mobilized. Part of the amygdala was removed after the incision on the medial side of the uncinate fasciculus was completed. Finally, the head of the hippocampus can be exposed in the temporal horn (images in the lower row)(images courtesy of AL Rhoton, Jr).
Click here to view the interactive module and related content for this image.
Figure 3: A coronal section through the right temporal lobe demonstrates the route of SA (left upper image). The fissure is generously split (right upper image) and the anterior portion of the inferior insular (limiting) sulcus has been identified (left middle image). An incision in the inferior limiting sulcus finds the temporal horn, hippocampus, choroid plexus, collateral eminence, and roof of the temporal horn (right middle image). The transchoroidal approach through the tenia fimbriae and removal of the hippocampus exposes the contents of the basal cisterns (photos in the lower row)(images courtesy of AL Rhoton, Jr).
TRANSSYLVIAN SELECTIVE AMYGDALOHIPPOCAMPECTOMY
There are three commonly described approaches for SA. The subtemporal approach was developed in an attempt to avoid unnecessary damage to the lateral temporal lobe. The transcortical approach via the middle temporal gyrus is technically simpler, with the drawback of damage to the lateral temporal neocortex. Finally, the transssylvian approach is the third surgical option and my preferred approach. Although technically more difficult, this approach spares the lateral temporal lobe structures interrupted during the transcortical approach and requires minimal retraction, unlike the subtemporal route.
The transsylvian SA as described by Yaşargil is accomplished through a standard pterional craniotomy. The patient is placed on the operating room table in a supine position. The patient’s head is rotated approximately 30 degrees toward the contralateral side and extended until the zygoma reaches the highest point on the face. This arrangement allows for gravity retraction of the frontal lobe and prevents the temporal cortex from obscuring the transsylvian operative corridor.
After the bone flap is elevated, the orbital roof is flattened and both the greater and lesser wings of the sphenoid wing are drilled away to the level of the superior orbital fissure. These latter maneuvers minimize retraction on the frontotemporal opercula and provide more flexible anterior operative working angles through the transsylvian route.
The dissection of the Sylvian fissure is described in the Technique of Sylvian Fissure Split chapter. Care should be taken to minimize manipulation of the MCA branches during the entire operation and thus decrease the risk of postoperative vasospasm. Papaverine-soaked gelfoam pledgets may be placed on these vessels to relieve their vasospasm if necessary.
INTRADURAL PROCEDURE
The following steps describe the intradural techniques for SA.
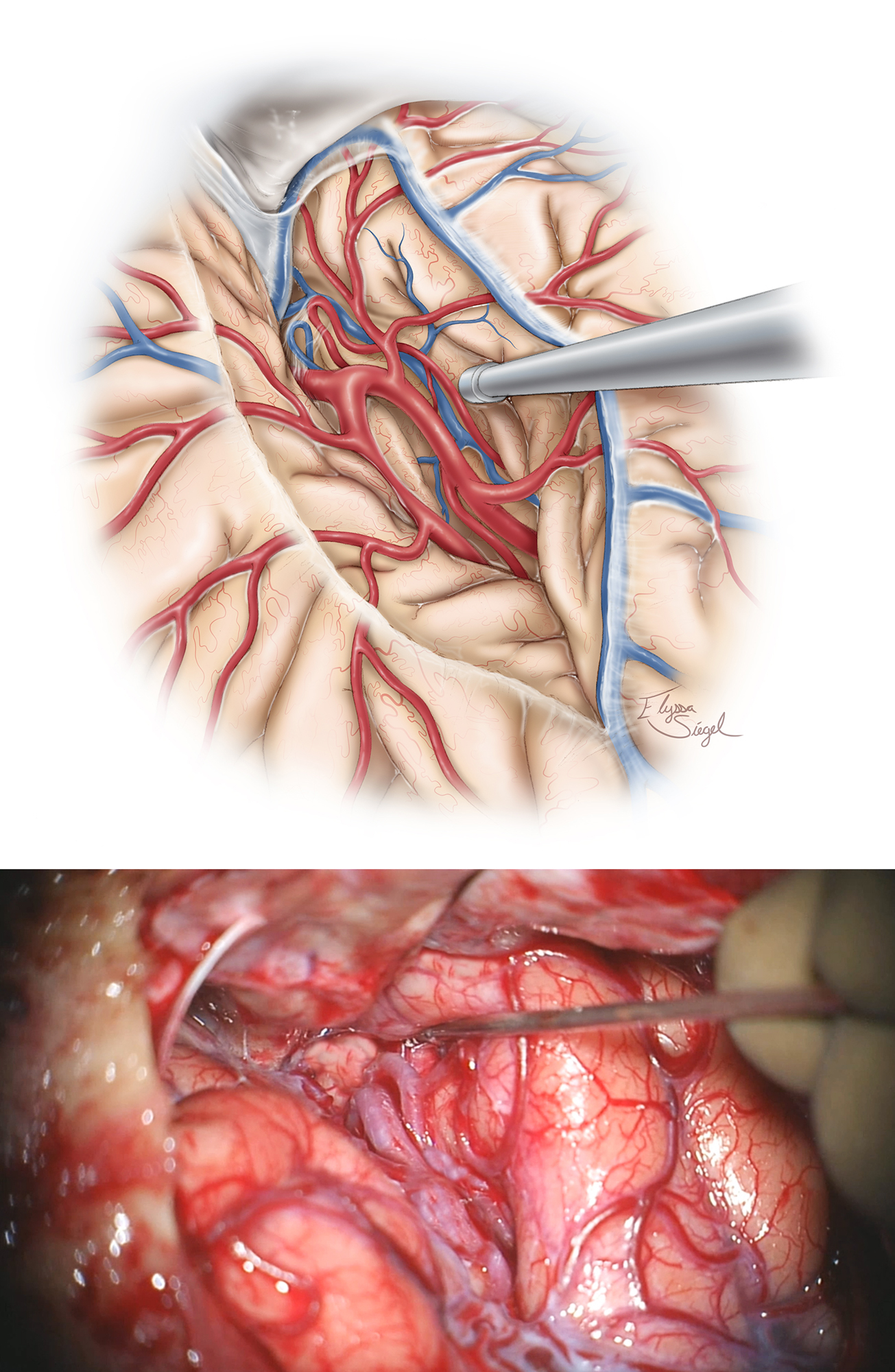
Figure 4: Retraction on the frontotemporal opercula should also be kept to a minimum throughout the procedure, and rigid retractors should be avoided to minimize the risks of retraction injury and venous infarction. Dynamic retraction using the hand-held suction device and wide arachnoid dissection is mandatory. Intrasylvian dissection is extended toward the temporal lobe and limen insulae as the inferior insular sulcus and vein are exposed along the temporal stem.
Amygdalohippocampectomy

Figure 5: Following identification of the M1 and proximal M2 branches and generous exposure of the inferior insula and temporal stem, I make the initial cortical incision in the inferior insular sulcus (10-20 millimeters), starting just posterior to or around the temporopolar artery and lateral to the inferior parassylvian vein, which should be coagulated. This incision is also guided by navigation. The approximate location of the underlying temporal horn and the hippocampus are noted (top illustration).

Figure 6: Incising the temporal stem allows access to the temporal horn, ultimately creating the corridor through which both the amygdala and hippocampus can be viewed. The temporal horn may not be immediately apparent due to the collapse of this part of the ventricle caused by release of cerebrospinal fluid (CSF) at the beginning of the procedure. The white matter dissection is performed in an oblique plane and can be disorienting, I routinely use neuronavigation to guide this part of dissection and removal of the lateral aspect of the amygdala to expose the anterior temporal horn.
Medially, the amygdala extends to the basal cisterns (chiasmatic, crural, and ambient) as the uncus. The uncus is divided into several segments. The semilunar gyrus (or the anterosuperior aspect of the uncus) represents the cortical projection of the amygdala, whereas the intralimbic gyrus (or posterior aspect of the uncus) represents the cortical projection of the hippocampus. The entorhinal sulcus and the optic tract separate the semilunar gyrus from the anterior perforated substance, the lateral margin of which is formed by the limen insulae.

Figure 7: The entire amygdala is carefully removed using an ultrasonic aspirator, bipolar cautery, and suction. This maneuver brings the hippocampus (middle image), medial tentorium (blue arrow) and the oculomotor nerve (yellow arrow)(lower image) into view through the remaining arachnoid membranes. An imaginary line that connects the MCA bifurcation to the anterior edge of the choroid plexus defines the superior border of the amygdala.

Figure 8: The anterior hippocampus (pes) is now safely separated and removed in a posterior-to-anterior direction. The body and tail of the hippocampus are removed in a second step. A very steep anterior-to-posterior operative trajectory is necessary to reach the posterior hippocampus.

Figure 9: The techniques for removal of the hippocampus are similar to those described above for the amygdala. Resection is conducted along the subpial planes lateral to the choroid plexus and superior to the arachnoid membranes along the basal cisterns; these membranes are protected while the parahippocampus is excised in a subpial manner. The anterior choroidal artery is not exposed. The posterior cerebral artery (PCA)(red arrow) is protected and its perforators (black arrow) entering the posterior hippocampus are isolated within the collateral sulcus, coagulated, and cut. Their avulsion injury is avoided.

Figure 10: A thin rim of brain tissue may be left along the lateral aspect of the choroid plexus and on the arachnoid layers of the basal cisterns to avoid injury to the brainstem and diencephalic structures (top sketch). Note the minimal invasion of the anatomy at the conclusion of the dissection.
The operative working distance for SA is narrow and long, and any injury to the MCA branches during aggressive retraction or manipulation should be avoided. The shaft of the microsurgical instruments may be used as dynamic retractors. Generous opening of the Sylvian fissure during the earlier stages of the operation avoids the need for aggressive retraction of the frontotemporal opercula. The medial edge of the tentorium remains a reliable landmark to protect the structures in the basal cisterns. Significant tension on the arachnoid layers along the edge of the tentorium may lead to temporary postoperative diplopia related to neuropraxia of the trochlear nerve.
Potential Complications
Meticulous handling of the superficial Sylvian veins decreases the risk of venous injury and resultant infarction. There is often a need for extensive microdissection through the Sylvian fissure and mobilization of the MCA’s temporal trunk to create additional operative space for the cortical incision along the inferior parainsular sulcus to enter the ventricle. These maneuvers may be risky if the principles of microsurgery are not carefully respected. Undue retraction on the frontotemporal opercula may lead to language dysfunction in the dominant hemisphere. Perforators from the temporal trunk of the MCA may be injured if these vessels are placed under undue tension.
Cerebral vasospasm: One of the most frequently discussed postoperative complications of SA is cerebral vasospasm resulting from subarachnoid bleeding within the operative field and aggressive manipulation of the corresponding vessels. The skill of the surgeon in navigating the complex anatomy of the temporal lobe while minimizing blood loss and vessel manipulation/retraction is paramount.
Visual field deficit: Similarly to ATL, visual field defects are common after SA. The defect manifests as a contralateral superior hemiquadrantanopia resulting from damage to the Meyer’s loop bending around the roof of the temporal horn of the lateral ventricle. The transsylvian approach via an incision made in the inferior insular sulcus at the level of the limen insulae or 5 mm just posterior would maximize protection of the optic radiations traversing the area.
If the surgeon is not intimately familiar with temporal lobe anatomy and microsurgical techniques and does not readily have access to neuronavigation, anteromedial neocortical removal followed by resection of medial structures is a reasonable alternative option.
Pearls and Pitfalls
- SA is an effective approach for removal of lesions located in the dominant amygdala and anterior hippocampus while preserving the normal anatomy.
DOI: https://doi.org/10.18791/nsatlas.v7.ch02.2
This chapter was previously presented in a similar format as part of the following publication:
Kovanda TJ, Tubbs RS, Cohen-Gadol AA. Transsylvian selective amygdalohippocampectomy for treatment of medial temporal lobe epilepsy: surgical technique and operative nuances to avoid complications.
Surg Neurol Int. 2014;12;5:133. PMID: 25298915
References
Adada B. Selective amygdalohippocampectomy via the transsylvian approach. Neurosurg Focus. 2008;25:E5.
Arruda F, Cendes F, Andermann F, Dubeau F, Villemure JG, Jones-Gotman M, et al. Mesial atrophy and outcome after amygdalohippocampectomy or temporal lobe removal. Ann Neurol. 1996;40:446-450.
Bate H, Eldridge P, Varma T, Wieshmann UC. The seizure outcome after amygdalohippocampectomy and temporal lobectomy. Eur J Neurol. 2007;14:90-94.
Berg AT, Langfitt J, Shinnar S, Vickrey BG, Sperling MR, Walczak T, et al. How long does it take for partial epilepsy to become intractable? Neurology. 2003;60:186-190.
Bonte FJ, Devous MD Sr, Stokely EM, Homan RW. Single-photon tomographic determination of regional cerebral blood flow in epilepsy. AJNR. Am J Neuroradiol. 1983;4:544-546.
Chelune GJ, Naugle RI, Luders H, Awad IA. Prediction of cognitive change as a function of preoperative ability status among temporal lobectomy patients seen at 6-month follow-up. Neurology. 1991;41:399-404.
Choi C, Rubino PA, Fernandez-Miranda JC, Abe H, Rhoton AL, Jr. Meyer's loop and the optic radiations in the transsylvian approach to the mediobasal temporal lobe. Neurosurgery. 2006;59:ONS228-235; discussion ONS235-236.
Clusmann H, Kral T, Gleissner U, Sassen R, Urbach H, Blumcke I, et al. Analysis of different types of resection for pediatric patients with temporal lobe epilepsy. Neurosurgery. 2004;54:847-859; discussion 859-860.
Clusmann H, Schramm J, Kral T, Helmstaedter C, Ostertun B, Fimmers R, et al. Prognostic factors and outcome after different types of resection for temporal lobe epilepsy. J Neurosurg. 2002;97:1131-1141.
de Tisi J, Bell GS, Peacock JL, McEvoy AW, Harkness WF, Sander JW, et al. The long-term outcome of adult epilepsy surgery, patterns of seizure remission, and relapse: a cohort study. Lancet. 2011;378:1388-1395.
Devous MD, Sr, Thisted RA, Morgan GF, Leroy RF, Rowe CC. SPECT brain imaging in epilepsy: a meta-analysis. J Nucl Med. 1998;39:285-293.
Dulay MF, Levin HS, York MK, Li X, Mizrahi EM, Goldsmith I, et al. Changes in individual and group spatial and verbal learning characteristics after anterior temporal lobectomy. Epilepsia. 2009;50:1385-1395.
Egan RA, Shults WT, So N, Burchiel K, Kellogg JX, Salinsky M. Visual field deficits in conventional anterior temporal lobectomy versus amygdalohippocampectomy. Neurology. 2000;55:1818-1822.
Engel J, Jr., McDermott MP, Wiebe S, Langfitt JT, Stern JM, Dewar S, et al. Early surgical therapy for drug-resistant temporal lobe epilepsy: a randomized trial. JAMA. 2012;307:922-930.
Engel J, Jr., Wiebe S, French J, Sperling M, Williamson P, Spencer D, et al. Practice parameter: temporal lobe and localized neocortical resections for epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003;60:538-547.
French JA, Williamson PD, Thadani VM, Darcey TM, Mattson RH, Spencer SS, et al. Characteristics of medial temporal lobe epilepsy: I. Results of history and physical examination. Ann Neurol. 1993;34:774-780.
Harvey DJ, Naugle RI, Magleby J, Chapin JS, Najm IM, Bingaman W, et al. Relationship between presurgical memory performance on the Wechsler Memory Scale-III and memory change following temporal resection for treatment of intractable epilepsy. Epilepsy Behav. 2008;13:372-375.
Helmstaedter C, Reuber M, Elger CC. Interaction of cognitive aging and memory deficits related to epilepsy surgery. Ann Neurol. 2002;52:89-94.
Hermann BP, Seidenberg M, Schoenfeld J, Davies K. Neuropsychological characteristics of the syndrome of mesial temporal lobe epilepsy. Arch Neurol. 1997;54:369-376.
Ho SS, Berkovic SF, Berlangieri SU, Newton MR, Egan GF, Tochon-Danguy HJ, et al. Comparison of ictal SPECT and interictal PET in the presurgical evaluation of temporal lobe epilepsy. Ann Neurol. 1995;37:738-745.
Hori T, Tabuchi S, Kurosaki M, Kondo S, Takenobu A, Watanabe T. Subtemporal amygdalohippocampectomy for treating medically intractable temporal lobe epilepsy. Neurosurgery. 1993;33:50-56; discussion 56-57.
Jones-Gotman M, Harnadek MC, Kubu CS. Neuropsychological assessment for temporal lobe epilepsy surgery. Can J Neurol Sci. 2000;27 Suppl 1:S39-43; discussion S50-52.
Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen Hauser W, Mathern G, et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51:1069-1077.
Lackner P, Koppelstaetter F, Ploner P, Sojer M, Dobesberger J, Walser G, et al. Cerebral vasospasm following temporal lobe epilepsy surgery. Neurology. 2012;78:1215-1220.
Mansouri A, Fallah A, Valiante TA. Determining surgical candidacy in temporal lobe epilepsy. Epilepsy Res Treat. 2012;2012:706917.
Mengesha T, Abu-Ata M, Haas KF, Lavin PJ, Sun DA, Konrad PE, et al. Visual field defects after selective amygdalohippocampectomy and standard temporal lobectomy. J Neuroophthal. 2009;29:208-213.
Mohammed HS, Kaufman CB, Limbrick DD, Steger-May K, Grubb RL, Jr., Rothman SM, et al. Impact of epilepsy surgery on seizure control and quality of life: a 26-year follow-up study. Epilepsia. 2012;53:712-720.
Morino M, Uda T, Naito K, Yoshimura M, Ishibashi K, Goto T, et al. Comparison of neuropsychological outcomes after selective amygdalohippocampectomy versus anterior temporal lobectomy. Epilepsy Behav. 2006;9:95-100.
Paglioli E, Palmini A, Portuguez M, Paglioli E, Azambuja N, da Costa JC, et al. Seizure and memory outcome following temporal lobe surgery: selective compared with nonselective approaches for hippocampal sclerosis. J Neurosurg. 2006;104:70-78.
Park TS, Bourgeois BF, Silbergeld DL, Dodson WE. Subtemporal transparahippocampal amygdalohippocampectomy for surgical treatment of mesial temporal lobe epilepsy. Technical note. J Neurosurg. 1996;85:1172-1176.
Radhakrishnan K, So EL, Silbert PL, Jack CR, Jr., Cascino GD, Sharbrough FW, et al. Predictors of outcome of anterior temporal lobectomy for intractable epilepsy: a multivariate study. Neurology. 1998;51:465-471.
Rausch R, Babb TL. Hippocampal neuron loss and memory scores before and after temporal lobe surgery for epilepsy. Arch Neurol 1993;50:812-817.
Rosenow F, Luders H. Presurgical evaluation of epilepsy. Brain. 2001;124:1683-1700.
Sagher O, Thawani JP, Etame AB, Gomez-Hassan DM. Seizure outcomes and mesial resection volumes following selective amygdalohippocampectomy and temporal lobectomy. Neurosurg Focus. 2012;32:E8.
Schaller C, Jung A, Clusmann H, Schramm J, Meyer B. Rate of vasospasm following the transsylvian versus transcortical approach for selective amygdalohippocampectomy. Neurol Res. 2004;26:666-670.
Schaller C, Zentner J. Vasospastic reactions in response to the transsylvian approach. Surg Neurol. 1998;49:170-175.
Semah F, Picot MC, Adam C, Broglin D, Arzimanoglou A, Bazin B, et al. Is the underlying cause of epilepsy a major prognostic factor for recurrence? Neurology. 1998;51:1256-1262.
Takaya S, Mikuni N, Mitsueda T, Satow T, Taki J, Kinoshita M, et al. Improved cerebral function in mesial temporal lobe epilepsy after subtemporal amygdalohippocampectomy. Brain. 2009;132:185-194.
Tanriverdi T, Olivier A. Cognitive changes after unilateral cortico-amygdalohippocampectomy unilateral selective-amygdalohippocampectomy mesial temporal lobe epilepsy. Turk Neurosurg. 2007;17:91-99.
Tubbs RS, Miller JH, Cohen-Gadol AA, Spencer DD. Intraoperative anatomic landmarks for resection of the amygdala during medial temporal lobe surgery. Neurosurgery. 2010;66:974-977.
Wen HT, Rhoton AL, Jr, de Oliveira E, Cardoso AC, Tedeschi H, Baccanelli M, et al. Microsurgical anatomy of the temporal lobe: part 1: mesial temporal lobe anatomy and its vascular relationships as applied to amygdalohippocampectomy. Neurosurgery. 1999;45:549-591; discussion 591-592.
Wendling AS, Hirsch E, Wisniewski I, Davanture C, Ofer I, Zentner J, et al. Selective amygdalohippocampectomy versus standard temporal lobectomy in patients with mesial temporal lobe epilepsy and unilateral hippocampal sclerosis. Epilep Res. 2013;104:94-104.
Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. New Engl J Med. 2001;345:311-318.
Wieser HG, Ortega M, Friedman A, Yonekawa Y. Long-term seizure outcomes following amygdalohippocampectomy. J Neurosurg. 2003;98:751-763.
Yasargil MG, Krayenbuhl N, Roth P, Hsu SP, Yasargil DC. The selective amygdalohippocampectomy for intractable temporal limbic seizures. J Neurosurg. 2010;112:168-185.
Zubal IG, Spencer SS, Imam K, Seibyl J, Smith EO, Wisniewski G, et al. Difference images calculated from ictal and interictal technetium-99m-HMPAO SPECT scans of epilepsy. J Nucl Med. 1995;36:684-689.
Related Materials
Available Through the Atlas
-

Microsurgical anatomy of the insula and the sylvian fissure
-
White matter fiber dissection of the optic radiations of the temp...
-
Modified approach for the selective treatment of temporal lobe ep...
-
Memory outcome following transsylvian selective amygdalohippocamp...
-
Selective amygdalohippocampectomy: The trans-middle temporal gyru...
-
Selective amygdalohippocampectomy via the transsylvian approach
-
Transsylvian hippocampal transection for mesial temporal lobe epi...
-
Transsylvian selective amygdalohippocampectomy for treatment of m...
Unavailable Through the Atlas
-

Meyer's loop and the optic radiations in the transsylvian approac...
-
Microsurgical Approaches to the Medial Temporal Region: An Anatom...
-
Differential effects of temporal pole resection with amygdalohipp...
-
Neuropsychological outcome after selective amygdalohippocampectom...
-
Advanced surgical approach for selective amygdalohippocampectomy...
-
Visual field defects in selective amygdalohippocampectomy for hip...
-
Neuropsychological outcome after selective amygdalohippocampectom...
-
Vascular events after transsylvian selective amygdalohippocampect...
-
Selective Amygdalohippocampectomy
Please login to post a comment.