

Vestibular Schwannoma

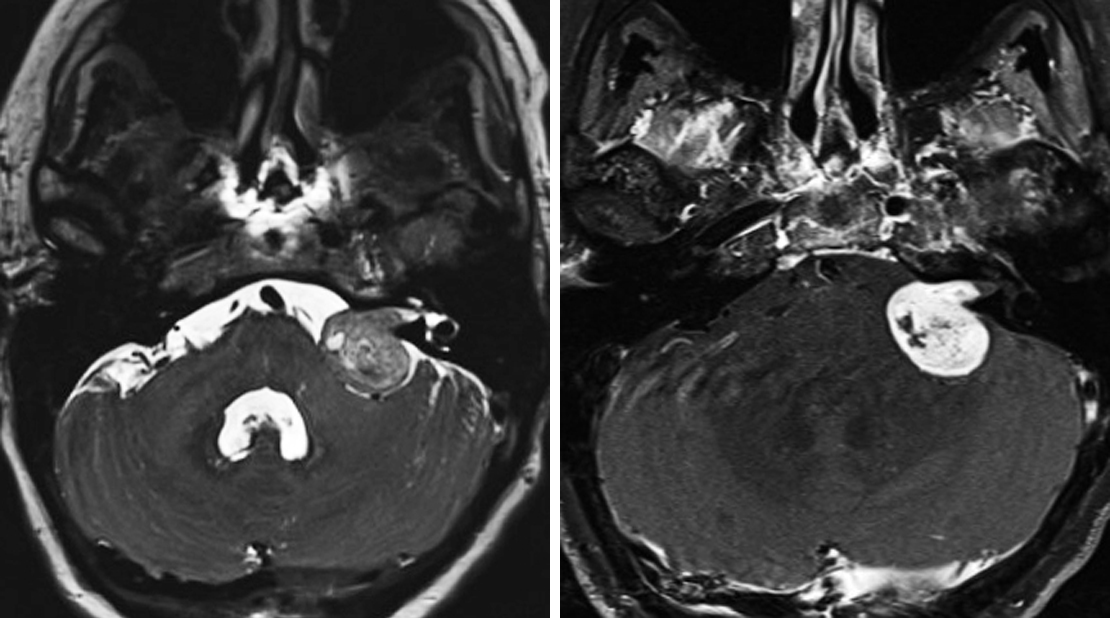
Figure 1: The most common intracranial location of schwannoma is the CPA, as in this patient. (Left) Cystic change is quite common in larger schwannomas on T2WI. (Right) Schwannomas are also typically avidly enhancing on postcontrast T1WI. This schwannoma can be differentiated from meningioma on the basis of this cystic change and the clearly delineated extension into the IAC. IAC remodeling and widening can also be present. The lack of a meningiomal "dural tail" is also helpful.

Figure 2: Axial T1-weighted postcontrast images demonstrate bilateral vestibular schwannomas (top left) and meningiomas (top right and middle left). Sagittal T1-weighted postcontrast (middle right) and T2-weighted (bottom) images demonstrate enhancing, expansile, centrally located intramedullary lesions within the spinal cord compatible with ependymomas in this patient with NF2.
![Figure 3: Postcontrast T1-weighted images (top left [axial] and top right [coronal]) demonstrate an avidly enhancing tiny schwannoma in the apex of the left IAC. (Bottom) A heavily T2-weighted CISS sequence also shows this nodule; this type of imaging can also show the nerve from which it arises. This appearance is typical for a tiny IAC schwannoma.](https://assets.neurosurgicalatlas.com/volumes/ATLAS/1-PRINCIPLES_OF_CRANIAL_SURGERY/02-Neuroradiology/03-BrainTumors/40-VS/PCS_NR_BT_VestSchwan_03.jpg)
Figure 3: Postcontrast T1-weighted images (top left [axial] and top right [coronal]) demonstrate an avidly enhancing tiny schwannoma in the apex of the left IAC. (Bottom) A heavily T2-weighted CISS sequence also shows this nodule; this type of imaging can also show the nerve from which it arises. This appearance is typical for a tiny IAC schwannoma.
BASIC DESCRIPTION
- Benign peripheral nerve sheath tumor arising from Schwann cells of cranial nerve (CN) VIII (vestibular portion) within the cerebellopontine angle-internal auditory canal (CPA-IAC)

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
PATHOLOGY
- WHO grade 1
- Originates from Schwann cells surrounding CN VIII vestibular segment
- CN VIII inferior vestibular branch > superior branch
- CN V and CN VII schwannomas not uncommon
- Origin in CN VIII cochlear portion is rare
- Bilateral vestibular schwannoma hallmark of neurofibromatosis type 2 (NF2)
- Mutations in NF2 tumor suppressor gene in majority of sporadic and familial cases
- Associated abnormality: arachnoid cyst or “CSF cap” (7%–10% of cases)
- Variable hypercellular (Antoni A) and more hypocellular (Antoni B) areas are characteristic microscopic features
- ±Intratumoral cysts, microhemorrhage
CLINICAL FEATURES
- Most common during adulthood (age 40–60 years)
- Uncommon in children unless associated with NF2
- Majority of cases exhibit slow growth over time
- Common presenting signs/symptoms: unilateral sensorineural hearing loss
- Treatment: surgical resection
- Prognosis: size >2 cm and involvement of IAC fundus and/or cochlear aperture are negative prognosticators for hearing preservation
IMAGING FEATURES
- General
- Well-marginated, enhancing mass within the CPA or CPA-IAC with “ice cream on cone” morphology
- Expansion of the IAC (in contrast to meningiomas)
- Small lesions can be entirely intracanalicular
- Calcification, cystic degeneration might be seen; hemorrhage rare
- CT
- Small lesions could be entirely intracanalicular and nonvisible on CT imaging
- Enhancement on contrast-enhanced CT imaging
- MRI
- T1WI: usually hypointense to isointense
- T2WI: high-resolution sequences (SPACE, CISS, or FIESTA) optimize visualization; appears as a hypo- to isointense CPA-IAC filling defect (ovoid if small, “ice cream on cone” if larger); ± hyperintense tumoral cysts
- T2*GRE: ±signal blooming from foci of microhemorrhage
- T1WI+C: avid enhancement
IMAGING RECOMMENDATIONS
- MRI without and with intravenous contrast, including high-resolution T2-weighted sequences through the CPA-IAC (SPACE, CISS, or FIESTA); serial MRI for small lesions to ensure stability
For more information, please see the corresponding chapter in Radiopaedia.
Contributors: Rachel Seltman, MD, and Jacob A. Eitel, MD
References
Furuta S, Takahashi S, Higano S, et al. Prediction of the origin of intracanalicular neoplasms with high-resolution MR imaging. Neuroradiology 2005;47:657–663. doi.org/10.1007/s00234-005-1400-x.
Osborn AG, Salzman KL, Jhaveri MD. Diagnostic Imaging (3rd ed). Elsevier, Philadelphia, PA; 2016.
Thamburaj K, Radhakrishnan VV, Thomas B, et al. Intratumoral microhemorrhages on T2*-weighted gradient-echo imaging helps differentiate vestibular schwannoma from meningioma. AJNR Am J Neuroradiol 2008;29:552–557. doi.org/10.3174/ajnr.A0887.
Woodruff JM, Kourea HP, Louis DN, et al. Schwannoma. In Kleihues P, Cavenee WK (eds), Tumours of the Nervous System. IARC Press, Lyon, France; 2000:164–166.
Zealley IA, Cooper RC, Clifford KM, et al. MRI screening for acoustic neuroma: a comparison of fast spin echo and contrast enhanced imaging in 1233 patients. Br J Radiol 2000;73:242–247. doi.org/10.1259/bjr.73.867.10817038.
Please login to post a comment.




