

Cortical Dysplasia


Figure 1: In this case, there is T1-isointense (top left), FLAIR-hyperintense (top right and bottom), nonenhancing signal within the left supramarginal and angular gyri subcortical white matter with overlying cortical thickening. Although cortical dysplasia can be a difficult diagnosis to make, it most commonly is perisylvian in location, as is seen in this case.
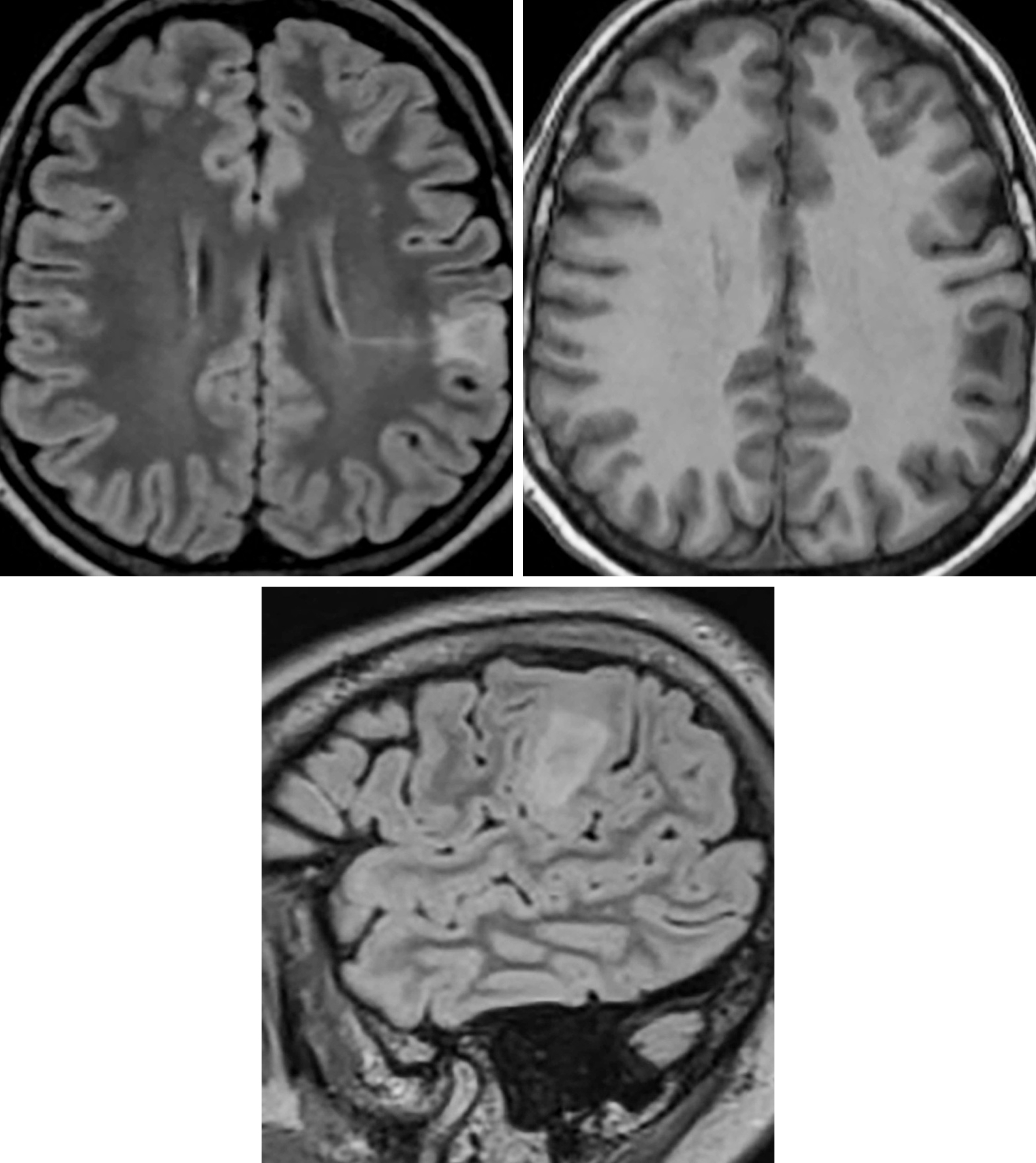
Figure 2: Although the Blumke classification is a pathologic classification, imaging occasionally will have features that are characteristic of type II cortical dysplasia (Taylor type). Notice the cortical and subcortical FLAIR-hyperintense and TI-hypointense signal with associated mild cortical expansion and a thin linear focus of FLAIR-hyperintense signal radiating toward the ventricle. This radiating signal is referred to as the transmantle sign.
Description
- Often associated with refractory epilepsy

ATLAS Choice Bipolar Forceps
Designed for your every surgical maneuver
Five tip sizes for brain and spine procedures
Unparalleled non-stick and low-profile features
Pathology
- Histologically classified based on giant dysmorphic neurons with or without balloon cells
Clinical Features
- Symptoms
- Refractory epilepsy
- Age and gender
- No gender predilection; usually manifests in the first 2 decades of life with seizures
Imaging
- General
- Thickening, blurring, and sometimes hyperintensity of the cortex
- Abnormal signal may be seen to extend from the cortex to the ventricle with tapering as it approaches the lateral ventricle
- Modality specific
- CT
- Usually normal
- MRI
- T1WI
- Slightly hypointense
- T2WI/FLAIR
- Homogeneous T2-hyperintense comet-tail
- Contrast
- Typically nonenhancing
- T1WI
- CT
- Imaging recommendations
- MRI with contrast
- Mimic
- Cortical dysplasia can mimic low-grade glioma, depending on its location, size, and configuration. Usually a triangular appearance with the apex toward the ventricle is more characteristic of transmantle dysplasia. The cortical thickening and blurring of dysplasia can be much more difficult to distinguish from low-grade tumor such as ganglioglioma.
For more information, please see the corresponding chapter in Radiopaedia.
Contributor: Sean Dodson, MD
References
Bronen RA, Vives KP, Kim JH, et al. Focal cortical dysplasia of Taylor, balloon cell subtype: MR differentiation from low-grade tumors. AJNR Am J Neuroradiol 1997;18:1141–1151.
Colombo N, Tassi L, Galli C, et al. Focal cortical dysplasias: MR imaging, histopathologic, and clinical correlations in surgically treated patients with epilepsy. AJNR Am J Neuroradiol 2003;24:724–733.
Rastogi S, Lee C, Salamon N. Neuroimaging in pediatric epilepsy: a multimodality approach. Radiographics 2008;28:1079–1095. doi.org/10.1148/rg.284075114
Please login to post a comment.




