

Trigeminal Schwannoma


This is a preview. Check to see if you have access to the full video. Check access
Trigeminal Schwannoma: Root Type
Trigeminal schwannomas are rare benign tumors representing the most common nonvestibular schwannoma, and 0.07 to 0.36% of all intracranial tumors. They may occur sporadically but case reports suggest patients with neurofibromatosis type 2 (NF-2) have an increased propensity to form these tumors in addition to the more commonly found vestibular schwannomas.
Schwannomas emerge from the peripheral nerve sheath, distal to the oligodendroglia–Schwann cell junction. The trigeminal nerve (cerebellpontine angle) and the gasserian ganglion (cavernous sinus and Meckel’s cave) are the most common sites for intracranial schwannomas after the vestibular nerve. Similar to vestibular schwannomas, gross-total resection of a trigeminal schwannoma portends a good prognosis regarding long-term tumor free survival; however, if only partial resection is achieved, recurrence is common.
The operative approach and difficulty of resection is highly dependent on the location of the tumor along the trigeminal nerve. Jefferson’s classification proposed in 1959, which categorized the tumor based on the segment of the nerve affected. The Jefferson classification schema categorizes tumors into four types. Root type tumors are those arising from the nerve root and involve the posterior fossa. Ganglion type tumors are those that originate from the gasserian ganglion and are confined to the middle fossa. Dumbbell tumors are larger tumors involving the middle and posterior fossa. The fourth type of tumor is division tumors, which involve the V1, V2, or V3 segment of the trigeminal nerve.
| Type | Description |
| Root |
Nerve root derived with posterior fossa involvement |
| Ganglion |
Gasserian ganglion derived with middle fossa involvement |
| Dumbbell |
Combination posterior fossa-middle fossa involvement |
|
Division
|
Peripheral segment involvement
|
Clinical Presentation
Patients with trigeminal schwannomas are nearly uniformly symptomatic with trigeminal nerve dysfunction at presentation. Symptoms typically include hypoesthesia within a variable distribution depending on the number of trigeminal segments affected. Keratitis can be an important feature heralding a loss of function within the trigeminal nerve due to the possible role of a diminished corneal reflex. Motor fibers of the nerve innervate the muscles of mastication including the tensor, digastric, and mylohyoid muscles with expected deficits in these muscles that are clinically rarely apparent. Trigeminal neuropathy follows an indolent course, corresponding to the slow-growth of the tumor.
Facial pain has also been reported in the setting of trigeminal schwannomas. The pain is different from the one experienced with trigeminal neuralgia. Although ticlike in onset, the long duration of pain and lack of a defined stimulus is characteristic of trigeminal schwannoma induced facial pain. These patients’ pain is also refractory to carbamazepine and other neuropathic pain medications used for trigeminal neuralgia. Despite this, the literature suggests that a small percentage of patients with trigeminal schwannomas experience pain consistent with the diagnosis of trigeminal neuralgia. All three divisions of the nerve are affected to different degrees at presentation.
Other presenting symptoms can be attributed to the mass effect on the surrounding cranial nerves. Deficits of facial motor, vestibular, and auditory function are possible with larger tumors. Diplopia is a result of compression on the oculomotor or abducens nerve, or from compression on the globe resulting in exophthalmos-related diplopia.
Evaluation
Patients with a trigeminal schwannoma should have a detailed neurologic examination with special consideration of trigeminal sensory and motor functions. A preoperative audiogram establishes the baseline functional status of cranial nerve (CN) VIII.
The complexity of the skull base anatomy relevant to resection of these tumors requires a thorough imaging evaluation. Magnetic resonance (MR) imaging characterizes the tumor’s size, degree of extension, and localizes the adjacent cranial nerves and cerebrovascular structures. Vestibular, facial and oculomotor schwannomas within the cerebellopontine angle can be difficult to differentiate from trigeminal schwannomas.
The radiographic evaluation includes computed tomography (CT) for defining the bony anatomy of the skull base and any resultant bony erosion. The proximity of the tumor to the carotid canal, cochlea, and internal auditory canal should be assessed to qualify the patient’s operative risk.
A CT angiogram defines the caliber of the involved arterial anatomy and elucidates the displacement of major vessels.

Figure 1: Schwannomas present as well-circumscribed, heterogeneously enhancing lesions that are isointense or hypointense on T1-weighted and hyperintense on T2-weighted images. They do not harbor the dural tail associated with meningiomas. Enlargement of the internal auditory meatus signifies a vestibular schwannoma. The MR images of the upper row indicate a classic trigeminal schwannoma with extension into the Meckel’s cave. The middle row demonstrates a giant tumor with intraorbital and extracranial or infratemporal extensions. The bottom photos show an isolated trigeminal schwannoma within the cerebellpontine angle.
Treatment
There are multiple management strategies for trigeminal schwannomas due to the benign slow-growing nature of these lesions. The most conservative approach is observation with serial imaging. This option includes a 6-12 month interval between the initial scans and is most applicable for patients with small tumors or elderly patients where the risk of surgery outweighs the risk of continued tumor growth.
Stereotactic radiosurgery is an option for small tumors with evidence of growth on serial imaging.
Microsurgical or endoscopic transnasal resection is the most definitive method of management for these lesions. If gross total resection is achieved, there is a low risk of recurrence, however, subtotal resection at the expense of preserving function can be supplemented with radiosurgery.
In the unique situation of bilateral trigeminal schwannomas, generally isolated to those patients with NF-2, the surgeon should only operate on the most symptomatic side. The contralateral nonsymptomatic tumor can be handled via observation or stereotactic radiosurgery.
Preoperative Considerations and Surgical Approach
The microsurgical or endoscopic approach utilized for trigeminal schwannomas is highly dependent upon the location of the tumor. The Jefferson’s classification simplifies the operative planning for these tumors. Table 2 lists the optimal surgical approaches for each type of tumor. Those tumors within the ganglion or peripheral category can be efficiently approached extradurally, to minimize the risk to adjacent cranial nerves.
| Type | Approach |
| Root | Retrosigmoid |
| Ganglion |
Extradural Subtemporal |
| Extradural Frontotemporal | |
| Dumbbell | Extradural Subtemporal |
| Extradural Subtemporal or Anterior Transpetrosal | |
| Extradural Modified Orbitozygomatic | |
| Combined Petrosal | |
|
Division
|
Modified Orbitozygomatic Pterional Extradural Subtemporal |
Because of the soft consistency of trigeminal schwannomas, gross total removal of large, multicompartment tumors with a predominantly middle fossa component is achievable via a single extradural approach through the middle fossa. This principle also holds true for tumors that harbor predominantly a posterior fossa extension whose middle fossa component can be extracted via a modified retrosigmoid corridor and opening over the expanded Meckel’s cave.
However, the reach of the posterior fossa corridor into the middle fossa is very limited. Therefore, tumors with equally dominant middle and posterior fossa extensions should undergo first a middle fossa surgery with an attempt to remove the entire tumor; a second stage retrosigmoid craniotomy may be needed if the posterior fossa component cannot be safely resected at the initial operation.
A lumbar drain, or alternatively an external ventricular catheter is placed preoperatively to facilitate brain relaxation. The use of neurophysiologic monitoring augments the surgeon’s efforts to preserve function. These monitoring tools include somatosensory evoked potentials (SSEPs) and brain stem auditory evoked responses (BAERs).
Operative Anatomy
The trigeminal nerve root originates from the lateral aspect of the rostral pons and travels superiorly, laterally, and anteriorly toward the petrous apex entering the Meckel's cave through the trigeminal impression, just inferior to the superior petrosal sinus. This first segment, which extends from the brainstem to the Meckel's cave, is referred to as the cisternal or cerebellopontine angle segment.
The root is myelinated by oligodendrocytes from its origin at the brainstem to the level of the central myelin–peripheral myelin transition zone, where the Schwann cells appear. Schwannomas arise from the peripheral myelin zone. After entering the trigeminal impression, the nerve courses within two leaflets of the dura, also known as the Meckel's cave.
Trigmeinal schwannomas involve the gasserian ganglion (middle fossa), the nerve root, (cerebellopontine angle) and the three divisions of the nerve (middle fossa). As expected, some tumors extend into more than one of these compartments and are typically dumbbell shaped. Rare tumors invade the extracranial space via the extracranial nerve branches in the orbit and infratemporal fossa. These tumors reach the orbit through the superior orbital fissure, and the infratemporal fossa through the foramen ovale or foramen rotundum.
The most frequent common tumor location is the middle cranial fossa (50%), followed by posterior fossa (30%) and dumbbell (20%) tumors. Extension into the cavernous sinus is common. These schwannomas do not infiltrate but rather displace their surrounding structures; therefore entry into the lateral cavernous sinus cavernous sinus for their removal is appropriate in most cases.
Click here to view the interactive module and related content for this image.
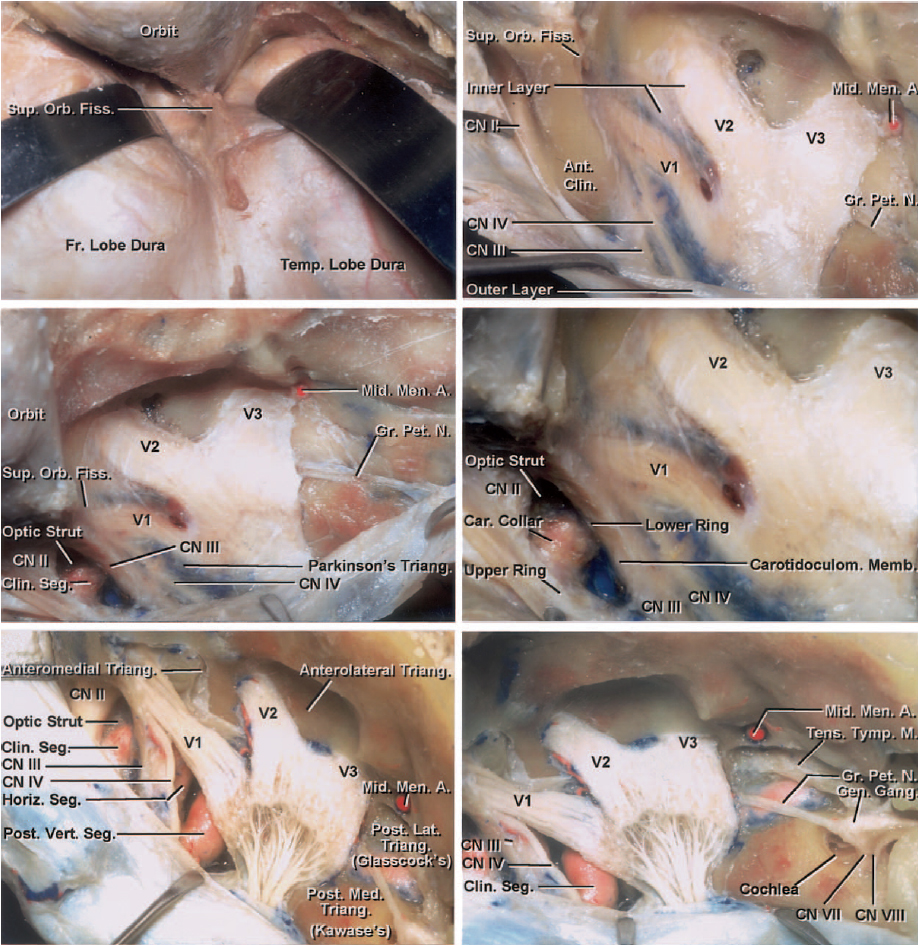
Figure 2: The extradural dissection of the cavernous sinus for removal of trigeminal schwannomas is indicated. An orbitozygomatic craniotomy and extradural clinoidectomy is necessary for this exposure (left upper image). The middle meningeal artery was sacrificed lateral to the posterior edge of V3. The outer wall of the cavernous sinus is peeled off from its inner layer after partial transection of the meningo-orbital dural band at the lateral edge of the superior orbital fissure. These maneuvers expose the nerves invested in the inner layer of the lateral wall as the meningeal (outer) layer is peeled away. Elevation of the middle fossa dura continues posteriorly and medially while the greater petrosal nerve is found (right upper image). The magnified view after extradural clinoidectomy is included (middle row). The inner dural layer of the lateral sinus wall is resected to expose the relevant structures that are usually displaced medially by the tumor. This maneuver is replaced by a linear incision over the tumor capsule, between and parallel to V1 and V2 divisions during surgery. The tumor expands the porus of the Meckel’s cave and creates a route toward the posterior fossa so the surgeon can deliver the component of the tumor within the cerebellopontine angle. The incision over the tumor can be extended into the posterior fossa dura over the bulk of the tumor capsule while coagulating and transecting the superior petrosal sinus. Note the approximate location of the middle fossa triangles (left lower image): the anteromedial triangle (between V1 and V2); the anterolateral triangle (between V2 and V3); the posterolateral triangle, also called Glasscock’s triangle (between V3 and the greater petrosal nerve); and the posteromedial triangle, also called Kawase’s triangle (lateral to the trigeminal nerve and posterior to the greater petrosal nerve). The petrous carotid is exposed under the greater petrosal nerve (images courtesy of AL Rhoton, Jr).

Click here to view the interactive module and related content for this image.
Figure 3: Anatomy of the trigeminal nerve over the Meckel’s cave is shown. The bone over the petrous ICA and surrounding structures has been removed to elucidate the location of these structures even though they are not exposed at surgery. These structures should be protected during microdissection. Note the need for disconnection of the superior petrosal sinus for reaching the cererbellopontine angle via the middle fossa exposure around the Meckel’s cave (images courtesy of AL Rhoton, Jr).

Click here to view the interactive module and related content for this image.
Figure 4: The anatomy of the trigeminal nerve originating from the brainstem is demonstrated. The origin of the trigeminal nerve is a reasonable landmark to define the border between the pons and the middle cerebellar peduncle (left upper image). The tentorium and the occipital lobe have been detached to expose the route of the trigeminal nerve through the trigeminal impression over the petrous apex (right upper image). The two motor rootlets of the trigeminal nerve, the superior and second inferior motor rootlets, are evident (left middle image). The dura of the anterior posterior fossa has been peeled away to uncover the basilar plexus, cavernous sinus, and inferior petrosal sinus. The Meckel’s cave is located at the trigeminal impression between the meningeal layer (dura propria) and the periosteal layer of the dura (right middle image). The superior petrosal sinus travels over the Meckel’s cave to join the cavernous sinus. Opening the roof of the Meckel’s caver requires clipping or coagulation of this sinus before its division to avoid venous bleeding (lower row).
RESECTION OF TRIGEMINAL SCHWANNOMA
Retrosigmoid Approach
The Extended retrosigmoid approach applies to root type tumors within the cerebellopontine angle. This approach is described in detail within the Retrosigmoid Craniotomy chapter.
The suprameatal tubercle is just above the internal acoustic meatus and posterior to the trigeminal nerve. Upon removal of the dura from the surface of the suprameatal tubercle and drilling the tubercle, additional exposure along the trigeminal nerve and above it is secured. Although helpful, this approach is rarely necessary.

Figure 5: A primarily cerebellopontine angle trigeminal schwannoma (upper row) is exposed via a right-sided retrosigmoid craniotomy (second row). Note the upper fascicles of the nerve engulfed by the tumor (yellow arow). The tumor is mobilized away from the brainstem (third row) and the attenuated nerve is carefully released (fourth row). Ultimately, most of the nerve was preserved (bottom photo).
Orbitozygomatic and Subtemporal Approaches
The orbitozygomatic craniotomy is optimally used for schwannomas involving different segmental distribution of the trigeminal nerve within the cavernous sinus. For a more detailed discussion, refer to the Orbitozygomatic Craniotomy chapter. If the surgeon requires a wider operative field for approaching a V1 lesion, the optic canal can be unroofed and an extradural anterior clinoidectomy performed.
The technical nuances of the subtemporal craniotomy are discussed in the Temporal/Subtemporal Craniotomy chapter. The extradural modification to this approach provides a particular advantage for this type of tumor.
This route is flexible and reaches middle fossa lesions that extend into the posterior fossa via traversing the Meckel’s cave. If the caliber of Meckel’s cave is insufficient to gain access into the posterior fossa, the exposure can be expanded via an incision in the dura of the Meckel’s that continues toward the superior petrosal sinus. Through extracapsular and intra-arachnoidal dissection, the posterior fossa portion of the tumor can be resected.
This approach also permits entry into the cavernous sinus via its lateral wall for resection of enclosed tumors, which are generally the larger sized trigeminal schwannomas. One caveat is the need to identify the petrous ICA to provide proximal control over the cavernous segment during the dissection. Intracavernous dissection requires minimal manipulation of the adjacent cranial nerves to avoid postoperative deficits. The tumor is internally debulked and its capsule mobilized circumferentially after sufficient debulking. This technique requires microdissection of the capsule away from the adjacent trigeminal fascicles. Part of the trigeminal nerve that is incorporated into the tumor is resected.

Figure 6: After completion of the orbitozygomatic craniotomy, the reflection of the temporal dura or the lateral wall of the cavernous sinus (the Kawase method) exposes the tumor covered by the inner cavernous wall dura. The meningo-orbital dural band at the lateral edge of the superior orbital fissure is partially transected and an extradural clinoidectomy is pursued. Elevation of the middle fossa dura continues posteriorly and medially while the greater petrosal nerve is found and sacrificed. A linear incision in the dura of the cavernous sinus, between and parallel to V1 and V2, unveils the tumor capsule. The tumor often expands the porus of the Meckel’s cave and creates a route toward the posterior fossa so the surgeon can deliver the component of the tumor within the cerebellopontine angle into the middle fossa resection cavity. The dural incision over the tumor can be extended into the posterior fossa over the bulk of the tumor capsule within the Meckel’s cave by coagulating and transecting the superior petrosal sinus.

Figure 7: An alternative method is the Dolenc approach that uses the oculomotor nerve as the center of attention for the entry point into the cavernous sinus. After an orbitozygomatic craniotomy and extradural clinoidectomy, the bone over the lateral and anterior aspect of the foramen rotundum and ovale is drilled to allow mobilization of these nerves within the foramina during tumor manipulation. The dura is incised along the Sylvian fissure and this dural incision is extended medially to the level of the distal or outer carotid ring. The distal ring is released and the anterior cavernous sinus is entered. The oculomotor nerve is found as it enters the edge of the tentorium. I open the dura over this nerve using an arachnoid knife. The trochlear nerve is posterolateral to the oculomotor nerve. The V1 is near the superior orbital fissure and is dissected from the overlying dura; this dissection along the nerve completes the exposure of the lateral wall of the cavernous sinus. The abducens nerve is the only nerve within the cavernous sinus and is immediately lateral to the ICA; it should be protected during dissection of the medial tumor capsule.

Figure 8: The tumor is debulked and dissected from the adjacent neurovascular structures within the cavernous sinus. Often, the V1 is the source of schwannoma and part of this nerve has to be sacrificed; the patient is most likely suffering from preoperative V1 numbness, therefore, allowing this maneuver.
Frontotemporal Approach
The frontotemporal or pterional craniotomy is applicable for small trigeminal schwannomas. This approach is described in more detail within the pterional Craniotomy chapter.
Anterior Petrosectomy Approach
The extradural subtemporal anterior transpetrous approach is described in more detail within the Anterior Petrosectomy chapter. This operative pathway is optimized for large multicompartment lesions with involvement of both the posterior and middle fossae.
Postoperative Considerations
During the early postoperative period, the patient will experience trigeminal neuropathy due to intraoperative manipulation of the nerve. This dysfunction will demonstrate gradual improvement during the postoperative period. Diminution or loss of the corneal reflex is of particular concern acutely, due to the risk for keratitis if this deficit goes unnoticed and proper eye care is not implemented timely.
Surgery of the cavernous sinus often requires manipulation of CNs III, IV, and VI. Therefore, postoperative diplopia from paresis of one or all of these CNs is not uncommon. These deficits are also generally transient and will improve within 3 months.
Pearls and Pitfalls
- Trigeminal schwannomas are a heterogeneous group of tumors because of the significant variations in their size, shape and location.
- Familiarity with a wide variety of skull base approaches is necessary for their optimal management.
Contributor: Benjamin K. Hendricks, MD
For additional illustrations of the combined middle-posterior fossa approach to Meckel's cave, please refer to the Jackler Atlas by clicking on the image below:

For additional illustrations of the middle fossa approach to Meckel's cave, please refer to the Jackler Atlas by clicking on the image below:

For additional illustrations of the posterior fossa approach to Meckel's cave, please refer to the Jackler Atlas by clicking on the image below:

References
Day JD. Surgical management of trigeminal neurinomas. In Badie B (ed), Neurosurgical Operative Atlas: Neuro-Oncology. Thieme Medical Publishers, Inc, New York, NY; 2007.
Gragnaniello C, Al-Mefty O, Kondziolka D, et al. Stereotactic radiosurgery for trigeminal schwannomas. In Al-Mefty O (ed), Controversies in Neurosurgery II. New York, NY: Thieme Medical Publishers, Inc; 2014.
Gragnaniello C, Al-Mefty O, Kondziolka D, et al. Total removal of trigeminal schwannomas. In Al-Mefty O (ed), Controversies in Neurosurgery II. New York, NY: Thieme Medical Publishers, Inc; 2014.
Raza SM, Amine MA, Anand V, et al. Endoscopic endonasal resection of trigminal schwannomas. Neurosurg Clin N Am 2015;26:473-479.
Sekhar LN, Sarma S, Schessel DA, et al. Nonvestibular Schwannomas of the Brain. In L.N. Sekhar & R.G. Fessler (Ed.), Atlas of Neurosurgical Techniques: Brain. Thieme Medical Publishers, Inc, New York, NY; 2006.
Related Materials
Available Through the Atlas
-

The Dolenc technique for cavernous sinus exploration (cadaveric p...
-
Trigeminal schwannomas: Results of Gamma Knife surgery in 37 case...
-
Surgical management of trigeminal schwannomas
-
Nonvestibular schwannoma tumors in the cerebellopontine angle: A...
-
Malignant peripheral nerve sheath tumors of the trigeminal nerve:...
-
Surgical management of trigeminal schwannomas: Defining the role...
Unavailable Through the Atlas
-

Microsurgical Anatomy and Approaches to the Cavernous Sinus
-
Microsurgical Anatomy of the Trigeminal Nerve
-
The surgical management of trigeminal neuromas
-
Nonvestibular schwannomas of the brain: A 7-year experience
-
Preservation of cranial nerve function after radiosurgery for non...
-
Stereotactic radiosurgery for trigeminal schwannomas
-
The subtemporal interdural approach to dumbbell-shaped trigeminal...
-
Trigeminal schwannomas: Experience with 68 cases
-
Trigeminal schwannomas: A report of 42 cases and review of the re...
-
Surgical treatment of intracavernous trigeminal schwannomas via a...
-
Trigeminal schwannomas: Experience with 57 cases and a review of...
-
Endoscopic endonasal approach for nonvestibular schwannomas
-
CyberKnife radiosurgery for Trigeminal Schwannomas
-
A critical evaluation of vestibular schwannoma surgery for patien...
Please login to post a comment.




